

Clinical Features and Management of Acquired Resistance to PD-1 Axis Inhibitors in 26 Patients With Advanced Non-Small Cell Lung Cancer
- PMID: 29578107
- PMCID: PMC6485248
- DOI: 10.1016/j.jtho.2018.03.008
Clinical Features and Management of Acquired Resistance to PD-1 Axis Inhibitors in 26 Patients With Advanced Non-Small Cell Lung Cancer
Abstract
Introduction: With expanding indications for programmed death 1 (PD-1) axis inhibitors in non-small cell lung cancer (NSCLC), acquired resistance (AR) to these therapies is increasingly being encountered. We sought to characterize clinical patterns of AR to PD-1 axis inhibitors in patients with advanced NSCLC, and evaluate subsequent outcome and management strategies for such patients.
Methods: Patients with NSCLC who developed AR to PD-1 axis inhibitor therapy initiated between December 2009 and February 2016 at one institution were identified and examined by clinical and radiographic features. AR was defined as progressive disease after initial response by either Response Evaluation Criteria in Solid Tumors v1.1 or immune-related response criteria.
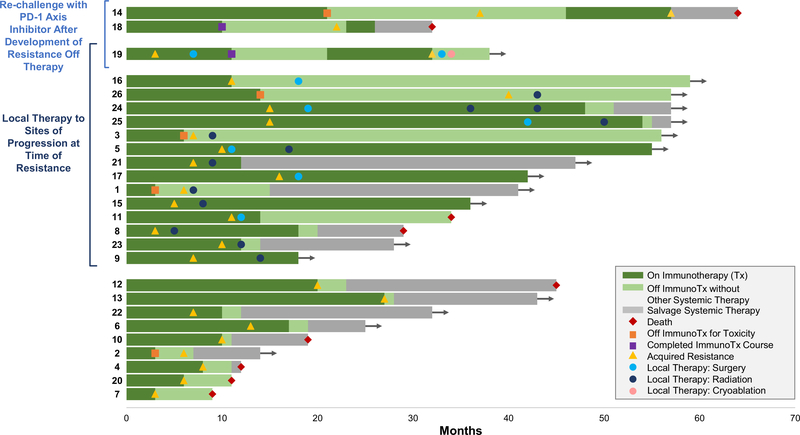
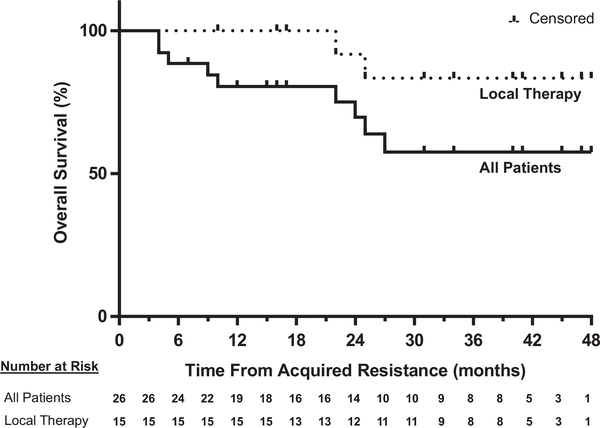
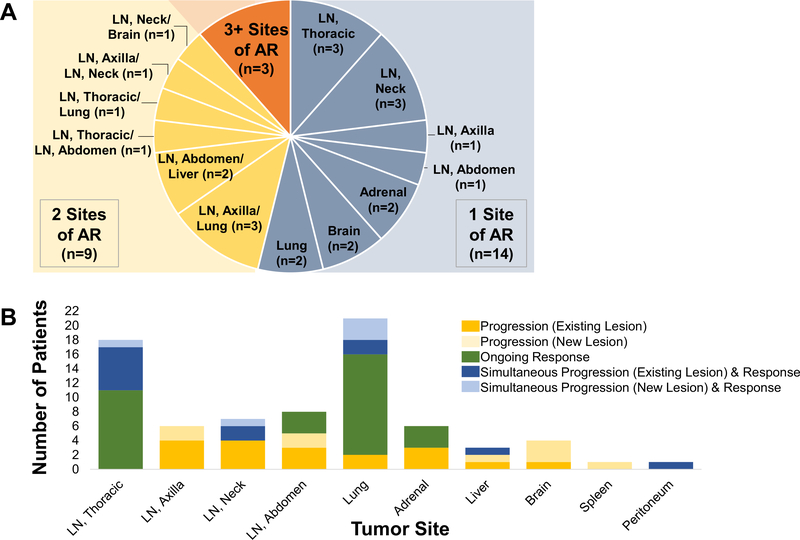
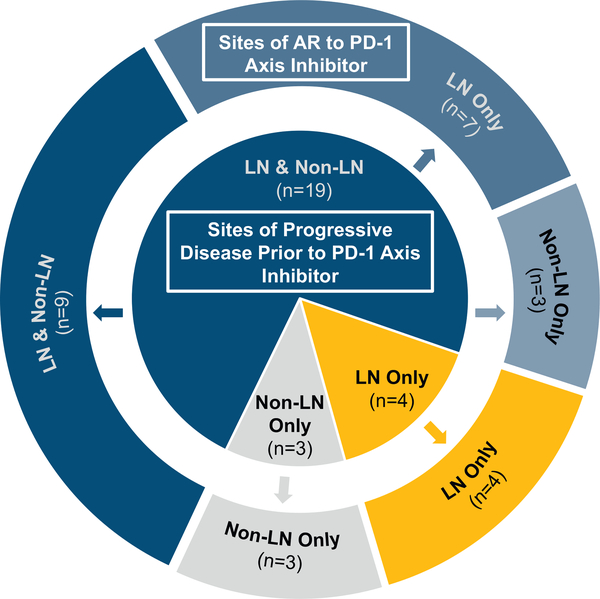
Results: Twenty-six patients with AR to PD-1 axis inhibitor therapy were identified and evaluated. Median time to AR was 313 days; the 2-year survival rate from AR was 70% (95% confidence interval: 0.53-0.92). Twenty patients (77%) experienced AR in lymph nodes (LNs), including 11 patients with LN-only progression. Twenty-three (88%) patients had recurrence limited to one (54%) or two (35%) sites of disease. Fourteen patients (54%) continued PD-1 axis inhibitor therapy beyond progression. Three patients were re-challenged with the same PD-1 axis inhibitor after holiday from and progression off therapy, 2 again responded. Fifteen patients (58%) received local therapy to site(s) of AR, 11 continued respective PD-1 axis inhibitor after local therapy. The 2-year survival rate from AR among these 15 patients was 92% (95% confidence interval: 0.77-1).
Conclusions: Acquired resistance to PD-1 axis inhibitors is often limited to one or two sites when local therapy and continuation of PD-1 axis inhibitor therapy can result in prolonged benefit. LN metastases appear to be particularly susceptible sites to AR. When progression of disease following response occurs after holiday from PD-1 axis inhibitor, re-challenge can again lead to tumor regression.
Keywords: PD-1; PD-L1; acquired resistance; immunotherapy; non–small cell lung cancer.
Copyright © 2018 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Perspectives on Acquired Resistance to PD-1 Axis Inhibitors in Patients with Non-Small Cell Lung Cancer.J Thorac Oncol. 2018 Jun;13(6):741-744. doi: 10.1016/j.jtho.2018.04.008. J Thorac Oncol. 2018. PMID: 29793645 No abstract available.
References
-
- Garon EB, Rizvi NA, Hui R, et al. Pembrolizumab for the treatment of non–small-cell lung cancer. N Engl J Med. 2015;372:2018–2028. - PubMed
-
- Barlesi F, Steins M, Horn L, et al. Long-term outcomes with nivolumab (Nivo) vs docetaxel (Doc) in patients (Pts) with advanced (Adv) NSCLC: CheckMate 017 and CheckMate 057 2-y update. Ann Oncol. 2016;27 (Suppl 6; Abstract 1215PD).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
