

Neurovascular sequestration in paediatric P. falciparum malaria is visible clinically in the retina
- PMID: 29578406
- PMCID: PMC5898913
- DOI: 10.7554/eLife.32208
Neurovascular sequestration in paediatric P. falciparum malaria is visible clinically in the retina
Abstract
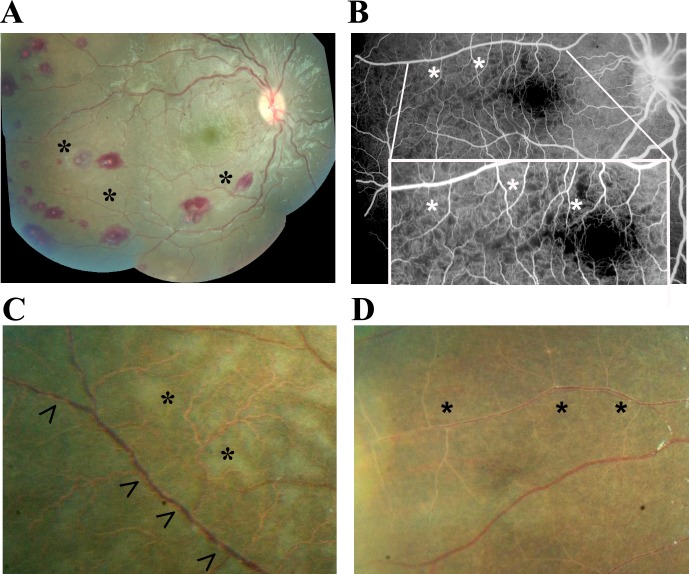
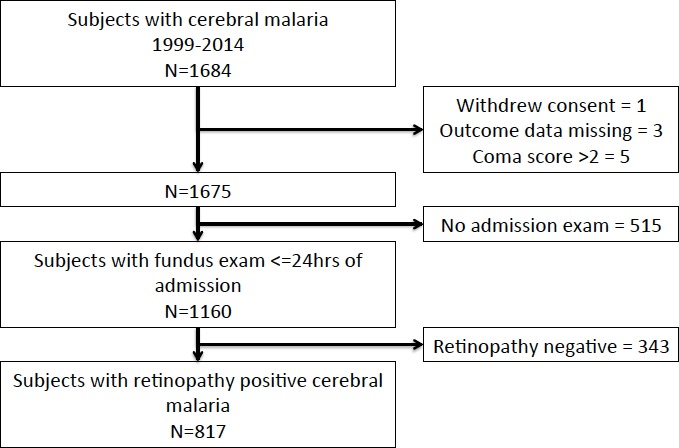
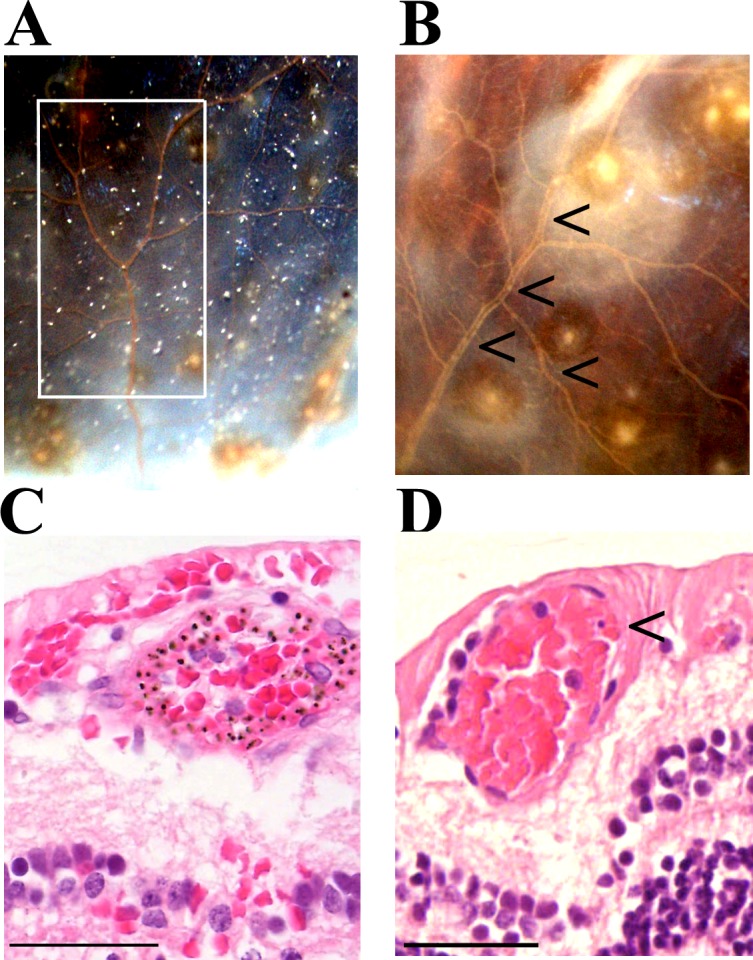
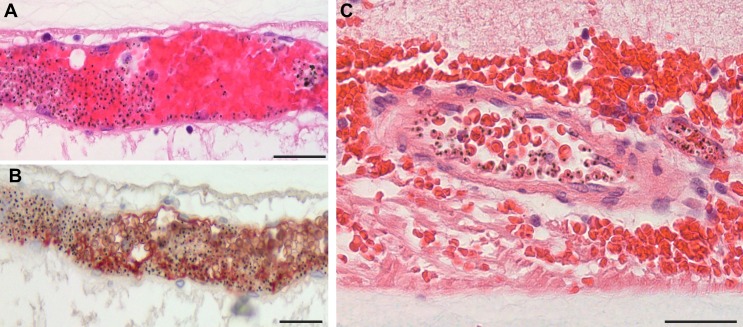
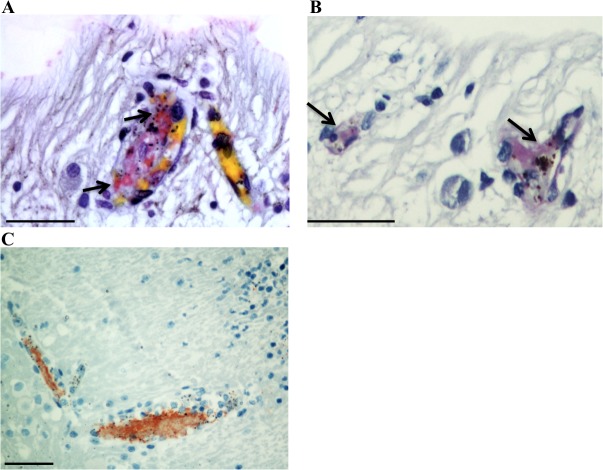
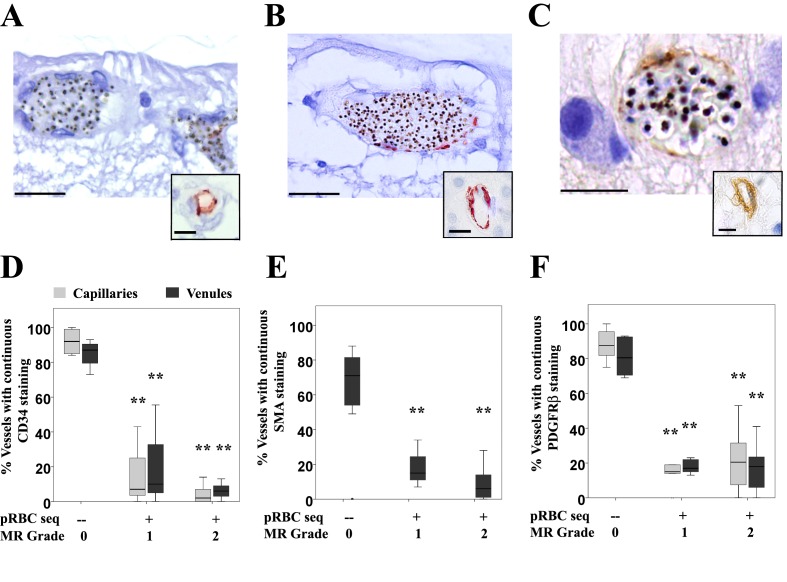
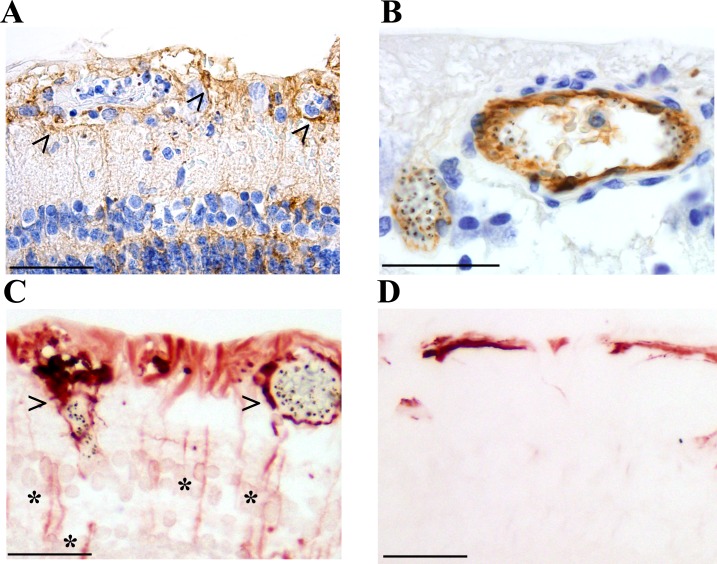
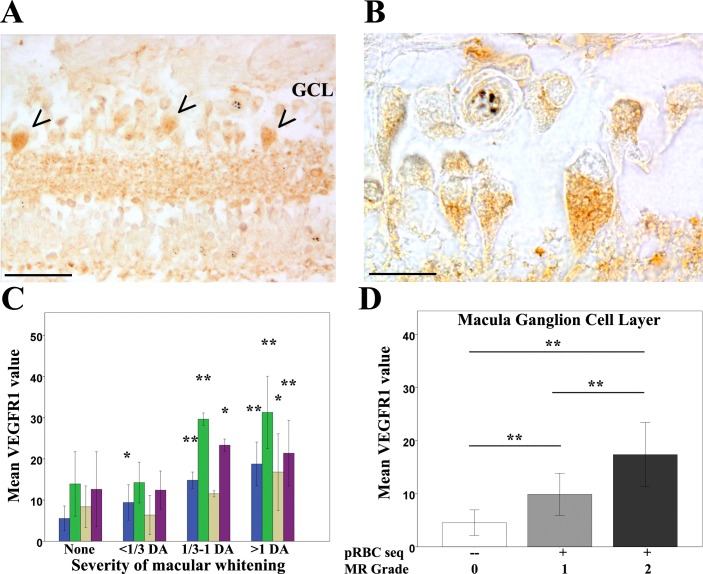
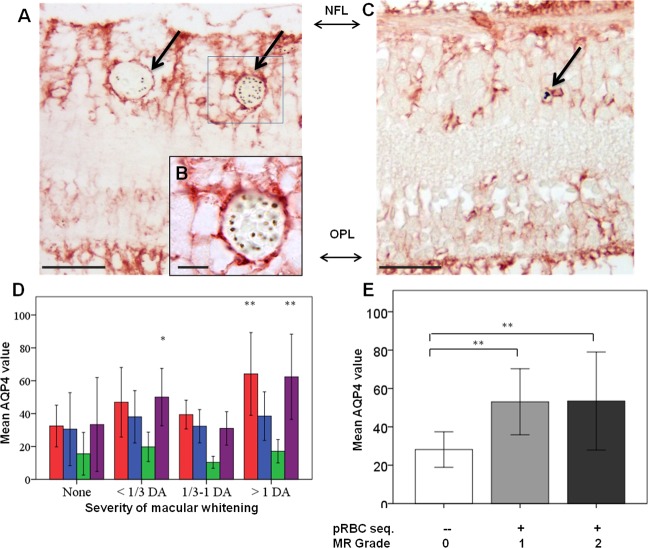
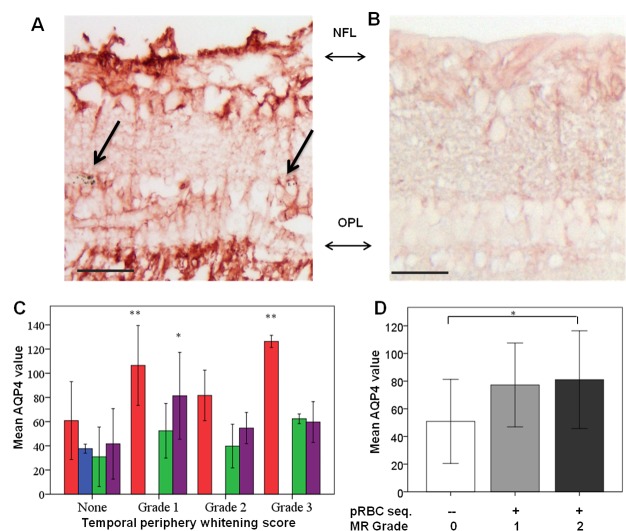
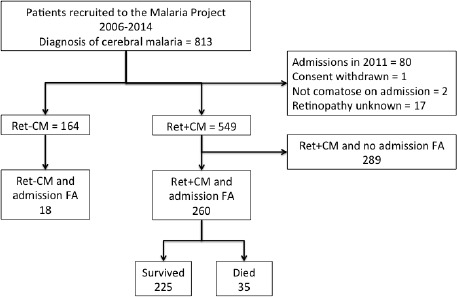
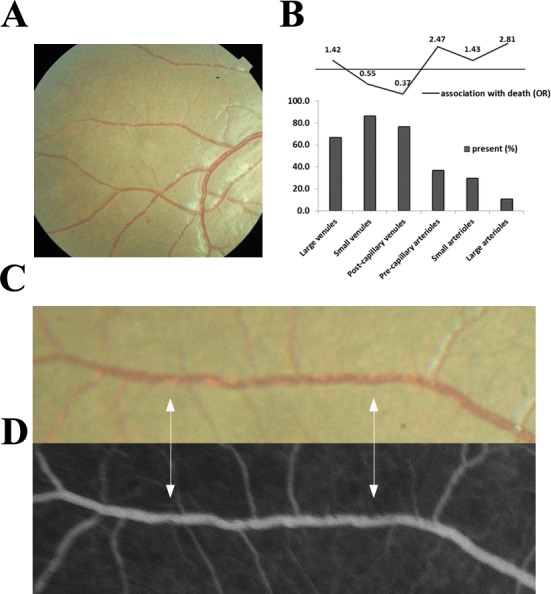
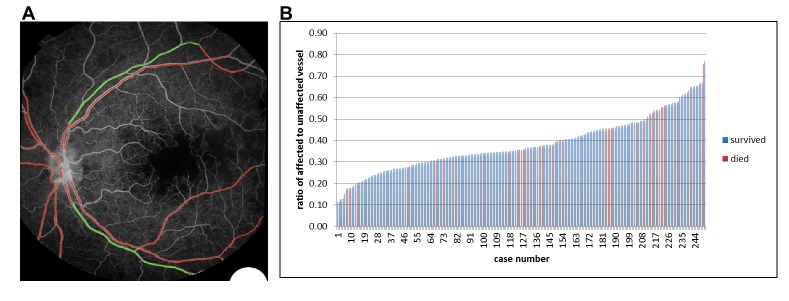
Retinal vessel changes and retinal whitening, distinctive features of malarial retinopathy, can be directly observed during routine eye examination in children with P. falciparum cerebral malaria. We investigated their clinical significance and underlying mechanisms through linked clinical, clinicopathological and image analysis studies. Orange vessels and severe foveal whitening (clinical examination, n = 817, OR, 95% CI: 2.90, 1.96-4.30; 3.4, 1.8-6.3, both p<0.001), and arteriolar involvement by intravascular filling defects (angiographic image analysis, n = 260, 2.81, 1.17-6.72, p<0.02) were strongly associated with death. Orange vessels had dense sequestration of late stage parasitised red cells (histopathology, n = 29; sensitivity 0.97, specificity 0.89) involving 360° of the lumen circumference, with altered protein expression in blood-retinal barrier cells and marked loss/disruption of pericytes. Retinal whitening was topographically associated with tissue response to hypoxia. Severe neurovascular sequestration is visible at the bedside, and is a marker of severe disease useful for diagnosis and management.
Keywords: P. falciparum; blood-retinal barrier; human; human biology; malarial retinopathy; medicine; neuroscience; neurovasculature; paediatric coma; plasmodium falciparum cerebral malaria; sequestration.
© 2018, Barrera et al.
Conflict of interest statement
VB, IM, GC, PH, VW, AC, NB, LC, YZ, SB, DM, SK, MM, TT, SH No competing interests declared
Figures
References
-
- Barrera V, Hiscott PS, Craig AG, White VA, Milner DA, Beare NA, MacCormick IJ, Kamiza S, Taylor TE, Molyneux ME, Harding SP. Severity of retinopathy parallels the degree of parasite sequestration in the eyes and brains of malawian children with fatal cerebral malaria. Journal of Infectious Diseases. 2015;211:1977–1986. doi: 10.1093/infdis/jiu592. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
