

Apixaban in patients at risk of stroke undergoing atrial fibrillation ablation
- PMID: 29579168
- PMCID: PMC6110196
- DOI: 10.1093/eurheartj/ehy176
Apixaban in patients at risk of stroke undergoing atrial fibrillation ablation
Abstract
Aims: It is recommended to perform atrial fibrillation ablation with continuous anticoagulation. Continuous apixaban has not been tested.
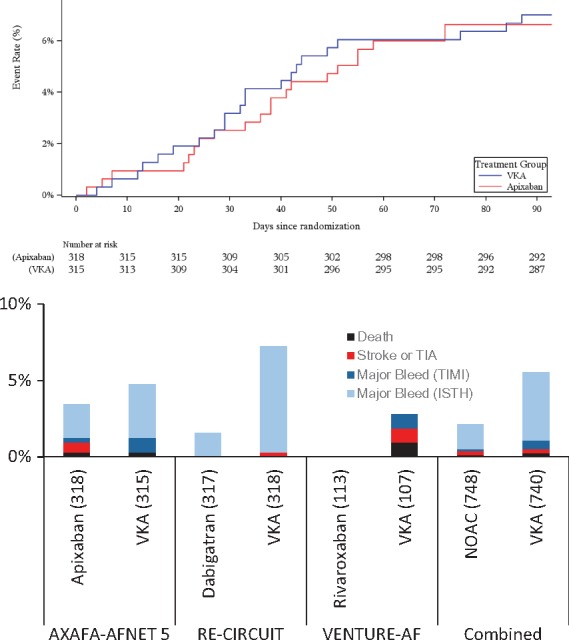
Methods and results: We compared continuous apixaban (5 mg b.i.d.) to vitamin K antagonists (VKA, international normalized ratio 2-3) in atrial fibrillation patients at risk of stroke a prospective, open, multi-centre study with blinded outcome assessment. Primary outcome was a composite of death, stroke, or bleeding (Bleeding Academic Research Consortium 2-5). A high-resolution brain magnetic resonance imaging (MRI) sub-study quantified acute brain lesions. Cognitive function was assessed by Montreal Cognitive Assessment (MoCA) at baseline and at end of follow-up. Overall, 674 patients (median age 64 years, 33% female, 42% non-paroxysmal atrial fibrillation, 49 sites) were randomized; 633 received study drug and underwent ablation; 335 undertook MRI (25 sites, 323 analysable scans). The primary outcome was observed in 22/318 patients randomized to apixaban, and in 23/315 randomized to VKA {difference -0.38% [90% confidence interval (CI) -4.0%, 3.3%], non-inferiority P = 0.0002 at the pre-specified absolute margin of 0.075}, including 2 (0.3%) deaths, 2 (0.3%) strokes, and 24 (3.8%) ISTH major bleeds. Acute small brain lesions were found in a similar number of patients in each arm [apixaban 44/162 (27.2%); VKA 40/161 (24.8%); P = 0.64]. Cognitive function increased at the end of follow-up (median 1 MoCA unit; P = 0.005) without differences between study groups.
Conclusions: Continuous apixaban is safe and effective in patients undergoing atrial fibrillation ablation at risk of stroke with respect to bleeding, stroke, and cognitive function. Further research is needed to reduce ablation-related acute brain lesions.
Figures





Comment in
-
Uninterrupted apixaban for atrial fibrillation ablation is a reasonable alternative, but what is the significance of silent cerebral infarctions?Eur Heart J. 2018 Aug 21;39(32):2956-2958. doi: 10.1093/eurheartj/ehy274. Eur Heart J. 2018. PMID: 29788351 No abstract available.
References
-
- Cosedis Nielsen J, Johannessen A, Raatikainen P, Hindricks G, Walfridsson H, Kongstad O, Pehrson S, Englund A, Hartikainen J, Mortensen LS, Hansen PS.. Radiofrequency ablation as initial therapy in paroxysmal atrial fibrillation. N Engl J Med 2012;367:1587–1595. - PubMed
-
- Verma A, Jiang CY, Betts TR, Chen J, Deisenhofer I, Mantovan R, Macle L, Morillo CA, Haverkamp W, Weerasooriya R, Albenque JP, Nardi S, Menardi E, Novak P, Sanders P.. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med 2015;372:1812–1822. - PubMed
-
- Kuck KH, Brugada J, Furnkranz A, Metzner A, Ouyang F, Chun KR, Elvan A, Arentz T, Bestehorn K, Pocock SJ, Albenque JP, Tondo C; Fire and ICE Investigators. Cryoballoon or radiofrequency ablation for paroxysmal atrial fibrillation. N Engl J Med 2016;374:2235–2245. - PubMed
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P, Agewall S, Camm J, Baron Esquivias G, Budts W, Carerj S, Casselman F, Coca A, De Caterina R, Deftereos S, Dobrev D, Ferro JM, Filippatos G, Fitzsimons D, Gorenek B, Guenoun M, Hohnloser SH, Kolh P, Lip GY, Manolis A, McMurray J, Ponikowski P, Rosenhek R, Ruschitzka F, Savelieva I, Sharma S, Suwalski P, Tamargo JL, Taylor CJ, Van Gelder IC, Voors AA, Windecker S, Zamorano JL, Zeppenfeld K.. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J 2016;37:2893–2962. - PubMed
-
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW.. Members AATF. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation 2014;130:e199–e267. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
