

Negligible Impact of Mass Screening and Treatment on Mesoendemic Malaria Transmission at West Timor in Eastern Indonesia: A Cluster-Randomized Trial
- PMID: 29579195
- PMCID: PMC6186863
- DOI: 10.1093/cid/ciy231
Negligible Impact of Mass Screening and Treatment on Mesoendemic Malaria Transmission at West Timor in Eastern Indonesia: A Cluster-Randomized Trial
Abstract
Background: Mass screening and treatment (MST) aims to reduce malaria risk in communities by identifying and treating infected persons without regard to illness.
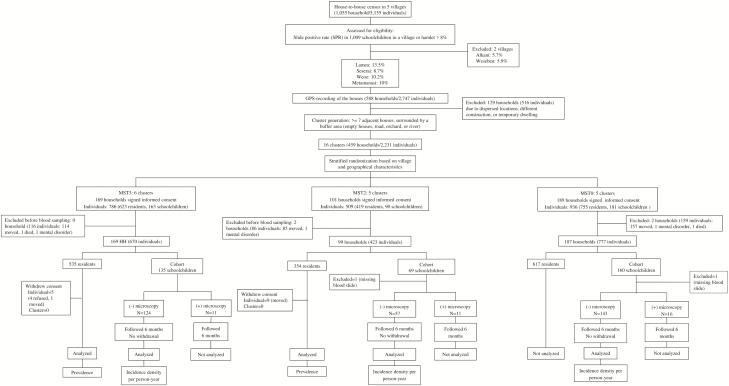
Methods: A cluster-randomized trial evaluated malaria incidence with and without MST. Clusters were randomized to 3, 2, or no MST interventions: MST3, 6 clusters (156 households/670 individuals); MST2, 5 clusters (89 households/423 individuals); and MST0, 5 clusters (174 households/777 individuals). All clusters completed the study with 14 residents withdrawing. In a cohort of 324 schoolchildren (MST3, n = 124; MST2, n = 57; MST0, n = 143) negative by microscopy at enrollment, we evaluated the incidence density of malaria during 3 months of MST and 3 months following. The MST intervention involved community-wide expert malaria microscopic screening and standard therapy with dihydroartemisinin-piperaquine and primaquine for glucose-6 phosphate dehydrogenase-normal subjects. All blood examinations included polymerase chain reaction assays, which did not guide on-site treatment.
Results: The risk ratios for incidence density of microscopically patent malaria in MST3 or MST2 relative to that in MST0 clusters were 1.00 (95% confidence interval [CI], .53-1.91) and 1.22 (95% CI, .42-3.55), respectively. Similar results were obtained with molecular analysis and species-specific (P. falciparum and P. vivax) infections. Microscopically subpatent, untreated infections accounted for 72% of those infected.
Conclusions: Two or 3 rounds of MST within 3 months did not impact the force of anopheline mosquito-borne infection in these communities. The high rate of untreated microscopically subpatent infections likely explains the observed poor impact.
Clinical trials registration: NCT01878357.
Figures



References
-
- World Health Organization. Global plan for artemisinin resistance containment. Geneva, Switzerland: WHO, 2011.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
