

Polygenic Risk Scores in Clinical Psychology: Bridging Genomic Risk to Individual Differences
- PMID: 29579395
- PMCID: PMC7772939
- DOI: 10.1146/annurev-clinpsy-050817-084847
Polygenic Risk Scores in Clinical Psychology: Bridging Genomic Risk to Individual Differences
Abstract
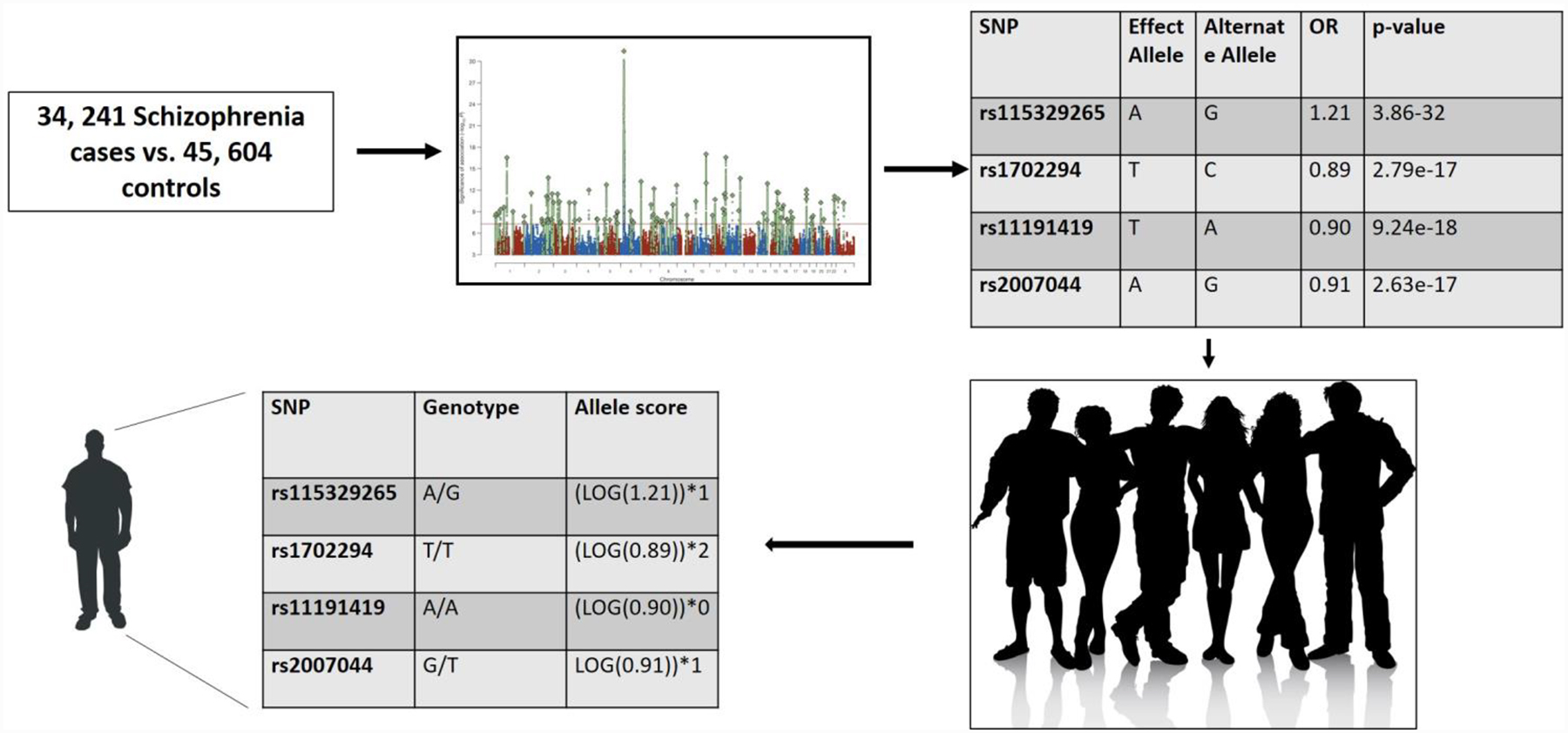
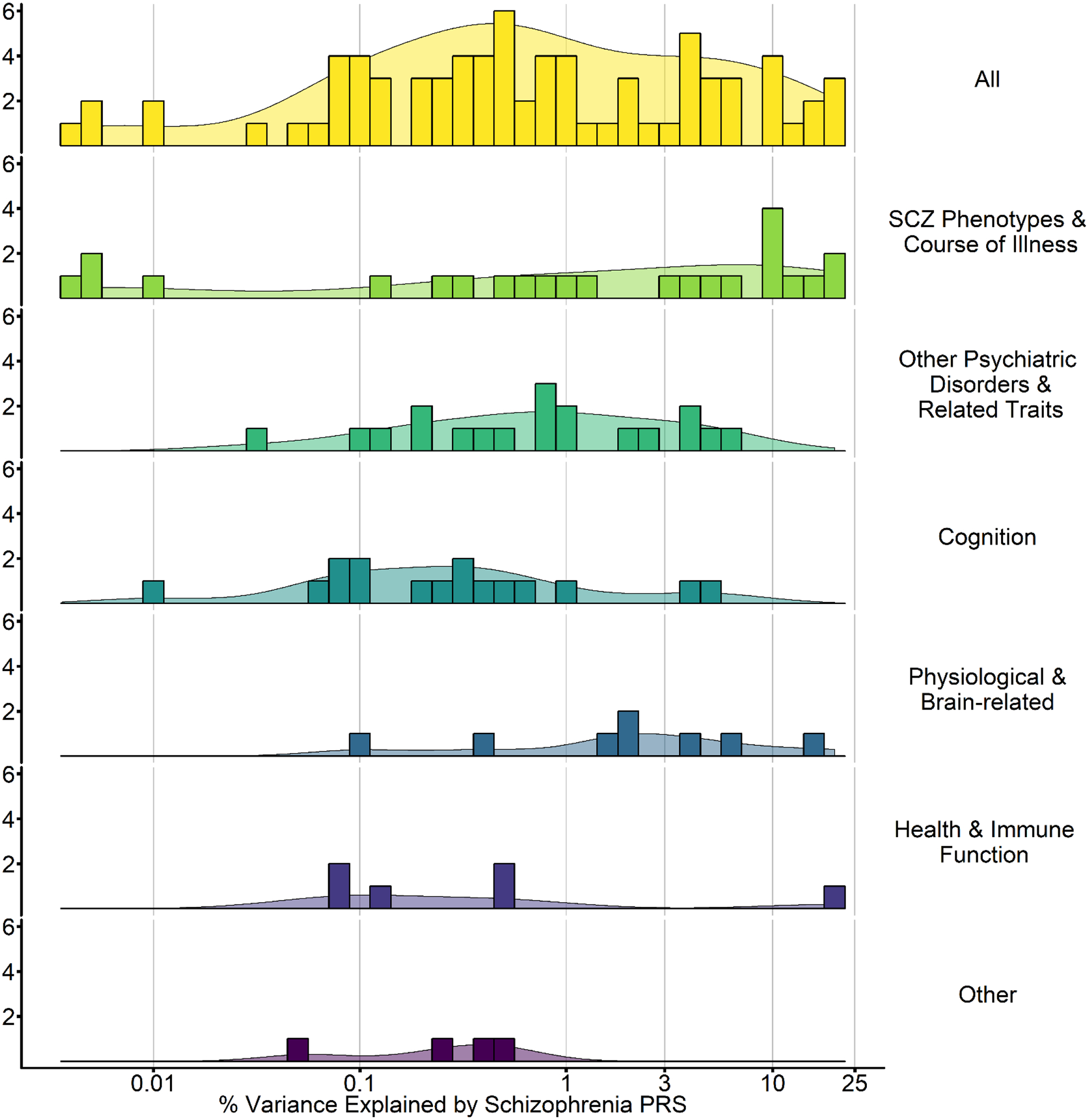
Genomewide association studies (GWASs) across psychiatric phenotypes have shown that common genetic variants generally confer risk with small effect sizes (odds ratio < 1.1) that additively contribute to polygenic risk. Summary statistics derived from large discovery GWASs can be used to generate polygenic risk scores (PRS) in independent, target data sets to examine correlates of polygenic disorder liability (e.g., does genetic liability to schizophrenia predict cognition?). The intuitive appeal and generalizability of PRS have led to their widespread use and new insights into mechanisms of polygenic liability. However, when currently applied across traits they account for small amounts of variance (<3%), are relatively uninformative for clinical treatment, and, in isolation, provide no insight into molecular mechanisms. Larger GWASs are needed to increase the precision of PRS, and novel approaches integrating various data sources (e.g., multitrait analysis of GWASs) may improve the utility of current PRS.
Keywords: GWAS; PRS; candidate; polygenic; psychopathology; schizophrenia.
Figures
References
-
- AAS M, MELLE I, BETTELLA F, DJUROVIC S, LE HELLARD S, BJELLA T, RINGEN PA, LAGERBERG TV, SMELAND OB, AGARTZ I, ANDREASSEN OA & TESLI M 2017. Psychotic patients who used cannabis frequently before illness onset have higher genetic predisposition to schizophrenia than those who did not. Psychol Med, 1–7. - PubMed
-
- AGERBO E, SULLIVAN PF, VILHJALMSSON BJ, PEDERSEN CB, MORS O, BORGLUM AD, HOUGAARD DM, HOLLEGAARD MV, MEIER S, MATTHEISEN M, RIPKE S, WRAY NR & MORTENSEN PB 2015. Polygenic Risk Score, Parental Socioeconomic Status, Family History of Psychiatric Disorders, and the Risk for Schizophrenia: A Danish Population-Based Study and Meta-analysis. JAMA Psychiatry, 72, 635–41. - PubMed
-
- AHN K, AN SS, SHUGART YY & RAPOPORT JL 2016. Common polygenic variation and risk for childhood-onset schizophrenia. Mol Psychiatry, 21, 94–6. - PubMed
-
- ANTTILA V, BULIK-SULLIVAN B, FINUCANE HK, BRAS J, DUNCAN L, ESCOTT-PRICE V, FALCONE G, GORMLEY P, MALIK R, PATSOPOULOS N, RIPKE S, WALTERS R, WEI Z, YU D, LEE P, BREEN G, BULIK C, DALY M, DICHGANS M, FARAONE S, GUERREIRO R, HOLMANS P, KENDLER K, KOELEMAN B, MATHEWS C, SCHARF J, SKLAR P, WILLIAMS J, WOOD N, COTSAPAS C, PALOTIE A, SMOLLER J, SULLIVAN P, ROSAND J, CORVIN A & NEALE B 2016. Analysis of shared heritability in common disorders of the brain. bioRxiv. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
