

Clinical impact of "pure" empirical catheter ablation of slow-pathway in patients with non-ECG documented clinical on-off tachycardia
- PMID: 29580297
- PMCID: PMC5870342
- DOI: 10.1186/s40001-018-0314-0
Clinical impact of "pure" empirical catheter ablation of slow-pathway in patients with non-ECG documented clinical on-off tachycardia
Abstract
Background: Catheter ablation of slow-pathway (CaSP) has been reported to be effective in patients with dual atrioventricular nodal conduction properties (dcp-AVN) and clinical ECG documentation but without the induction of tachycardia during electrophysiological studies (EPS). However, it is unknown whether CaSP is beneficial in the absence of pre-procedural ECG documentation and without the induction of tachycardia during EPS. The aim of this study was to evaluate long-term results after a "pure" empirical CaSP (peCaSP).
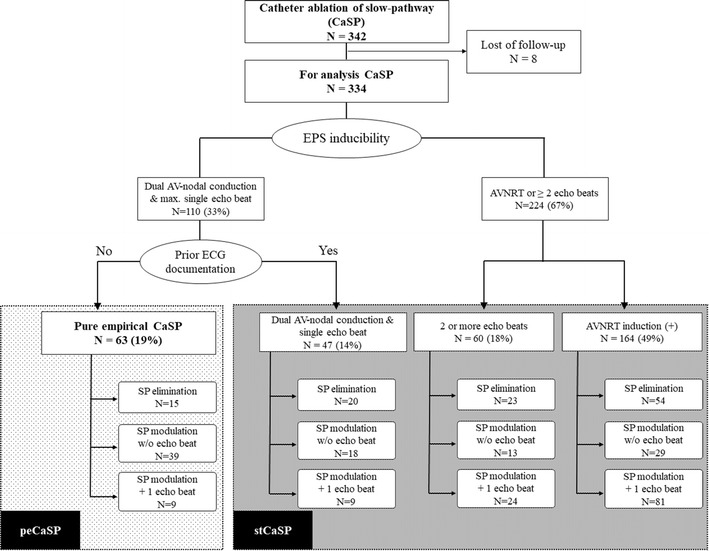
Methods: 334 consecutive patients who underwent CaSP (91 male, 47.5 ± 17.6 years) were included in this study. Sixty-three patients (19%) who had no pre-procedural ECG documentation, and demonstrated dcp-AVN with a maximum of one echo-beat were assigned to the peCaSP group. The remaining 271 patients (81%) were assigned to the standard CaSP group (stCaSP). Clinical outcomes of the two groups were compared, based on ECG documented recurrence or absence of tachycardia and patients' recorded symptoms.
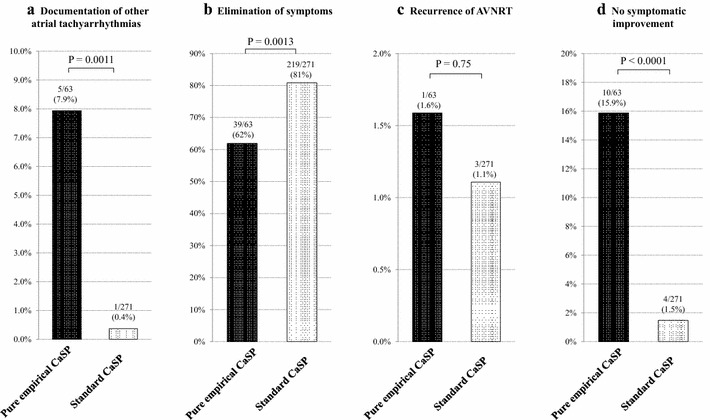
Results: CaSP was performed in all patients without any major complications including atrioventricular block. During follow-up (909 ± 435 days), 258 patients (77%) reported complete cessation of clinical symptoms. There was no statistically significant difference in the incidence of AVNRT recurrence between the peCaSP and stCaSP groups (1/63 [1.6%] vs 3/271 [1.1%], P = 0.75). Complete cessation of clinical symptoms was noted significantly less frequently in patients after peCaSP (39/63 [62%] vs 219/271 [81%], P = 0.0013). The incidence of non-AVNRT atrial tachyarrhythmias (AT) was significantly higher in patients after peCaSP (5/63 [7.9%] vs 1/271 [0.4%], P = 0.0011).
Conclusion: A higher incidence of other AT and subjective symptom persistence are demonstrated after peCaSP, while peCaSP improves clinical symptoms in 60% of patients with non-documented on-off tachycardia.
Keywords: AVNRT; ECG documentation; Empiric ablation; Slow-pathway ablation; Supraventricular tachycardia.
Figures
References
-
- Blomstrom-Lundqvist C, Scheinman MM, Aliot EM, Alpert JS, Calkins H, Camm AJ, Campbell WB, Haines DE, Kuck KH, Lerman BB, Miller DD, Shaeffer CW, Jr, Stevenson WG, Tomaselli GF, Antman EM, Smith SC, Jr, Alpert JS, Faxon DP, Fuster V, Gibbons RJ, Gregoratos G, Hiratzka LF, Hunt SA, Jacobs AK, Russell RO, Jr, Priori SG, Blanc JJ, Budaj A, Burgos EF, Cowie M, Deckers JW, Garcia MA, Klein WW, Lekakis J, Lindahl B, Mazzotta G, Morais JC, Oto A, Smiseth O, Trappe HJ, American College of Cardiology. American Heart Association Task Force on Practice Guidelines. European Society of Cardiology Committee for Practice Guidelines Writing committee to develop guidelines for the management of patients with supraventricular arrhythmias. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias—executive summary. Circulation. 2003;108:1871–1909. doi: 10.1161/01.CIR.0000091380.04100.84. - DOI - PubMed
-
- Page RL, Joglar JA, Caldwell MA, Calkins H, Conti JB, Deal BJ, Estes NA, 3rd, Field ME, Goldberger ZD, Hammill SC, Indik JH, Lindsay BD, Olshansky B, Russo AM, Shen WK, Tracy CM, Al-Khatib SM. 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2016;67:e27–e115. doi: 10.1016/j.jacc.2015.08.856. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
