

CKD Self-management: Phenotypes and Associations With Clinical Outcomes
- PMID: 29580660
- PMCID: PMC6109611
- DOI: 10.1053/j.ajkd.2018.01.047
CKD Self-management: Phenotypes and Associations With Clinical Outcomes
Abstract
Background: To slow chronic kidney disease (CKD) progression and its complications, patients need to engage in self-management behaviors. The objective of this study was to classify CKD self-management behaviors into phenotypes and assess the association of these phenotypes with clinical outcomes.
Study design: Prospective cohort study.
Setting & participants: Adults with mild to moderate CKD enrolled in the Chronic Renal Insufficiency Cohort (CRIC) Study. 3,939 participants in the CRIC Study recruited between 2003 and 2008 served as the derivation cohort and 1,560 participants recruited between 2013 and 2015 served as the validation cohort.
Predictors: CKD self-management behavior phenotypes.
Outcomes: CKD progression, atherosclerotic events, heart failure events, death from any cause.
Measurements: Latent class analysis stratified by diabetes was used to identify CKD self-management phenotypes based on measures of body mass index, diet, physical activity, blood pressure, smoking status, and hemoglobin A1c concentration (if diabetic); Cox proportional hazards models.
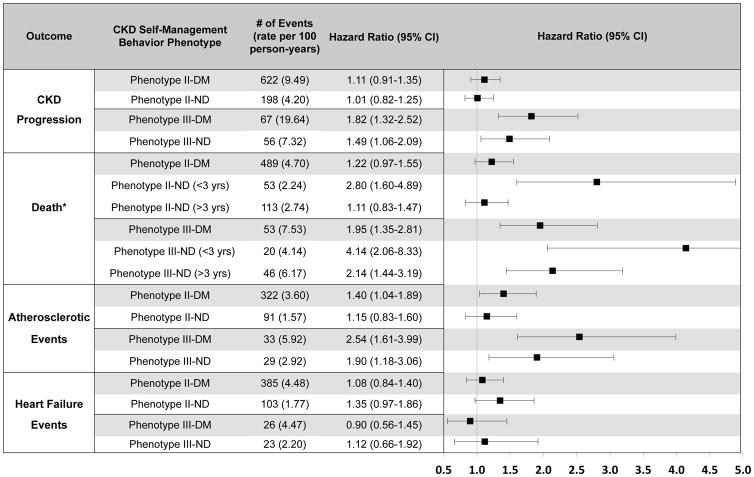
Results: 3 identified phenotypes varied according to the extent of implementation of recommended CKD self-management behaviors: phenotype I characterized study participants with the most recommended behaviors; phenotype II, participants with a mixture of recommended and not recommended behaviors; and phenotype III, participants with minimal recommended behaviors. In multivariable-adjusted models for those with and without diabetes, phenotype III was strongly associated with CKD progression (HRs of 1.82 and 1.49), death (HRs of 1.95 and 4.14), and atherosclerotic events (HRs of 2.54 and 1.90; each P < 0.05). Phenotype II was associated with atherosclerotic events and death among those with and without diabetes.
Limitations: No consensus definition of CKD self-management; limited to baseline behavior data.
Conclusions: There are potentially 3 CKD self-management behavior phenotypes that distinguish risk for clinical outcomes. These phenotypes may inform the development of studies and guidelines regarding optimal self-management.
Keywords: CKD progression: cardiovascular outcomes; Chronic renal failure; all-cause death; atherosclerotic events; blood pressure control; chronic kidney disease (CKD); diabetes; healthy behaviors; heart failure; modifiable risk factors; patient engagement; self-care; self-management; smoking.
Copyright © 2018 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Levey A, Coresh J. Chronic Kidney Disease. Lancet. 2012;379:165–180. - PubMed
-
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 suppl 1):S1–266. - PubMed
-
- MacGregor M, Taal M. Clinical Practice Guidelines: Detection, Monitoring and Care of Patients with CKD. (5) 2011:1–71. Available at: http://www.renal.org/guidelines. - PubMed
-
- National Kidney Foundation. K/DOQI Clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. Am J Kidney Dis. 2004;43(5 Suppl 1):S1–S290. - PubMed
-
- National Kidney Foundation. KDOQI Clinical Practice Guidelines for Diabetes and CKD: 2012 Update. Am J Kidney Dis. 2012;60:850–886. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 DK072231/DK/NIDDK NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- F32 DK113681/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- U54 GM104940/GM/NIGMS NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- UL1 TR002240/TR/NCATS NIH HHS/United States
- K23 DK094829/DK/NIDDK NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- U24 DK060990/DK/NIDDK NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- T32 DK007785/DK/NIDDK NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- P20 GM109036/GM/NIGMS NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- UL1 TR002003/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
