

Anti-CTLA-4 therapy requires an Fc domain for efficacy
- PMID: 29581255
- PMCID: PMC5899492
- DOI: 10.1073/pnas.1801524115
Anti-CTLA-4 therapy requires an Fc domain for efficacy
Abstract
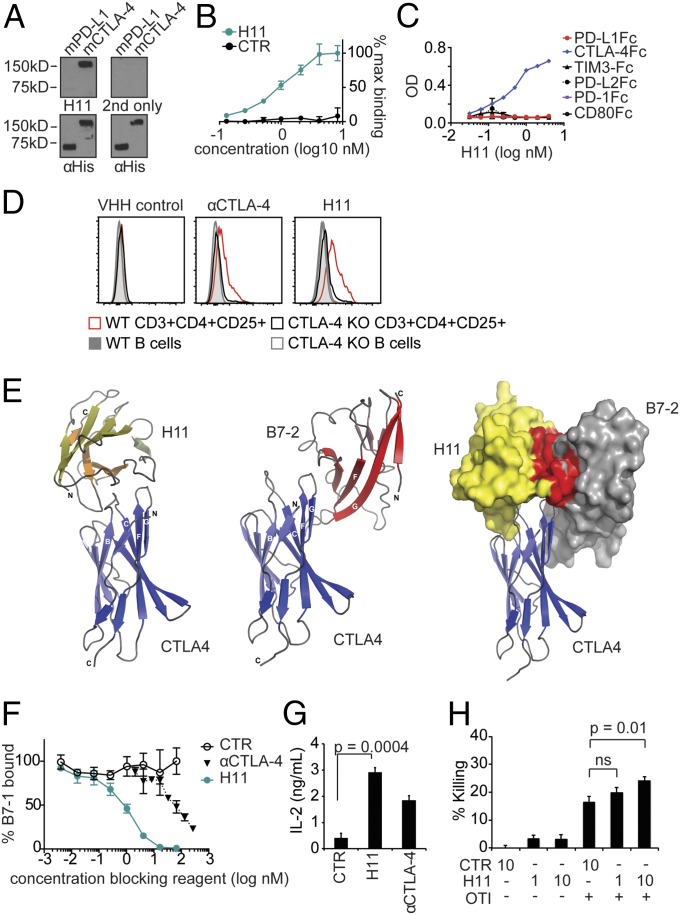
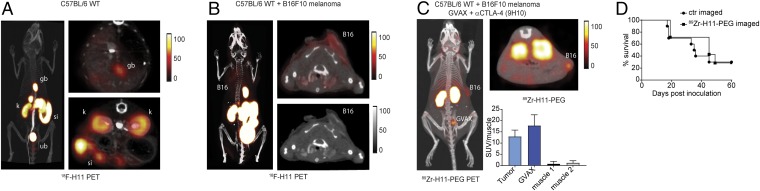
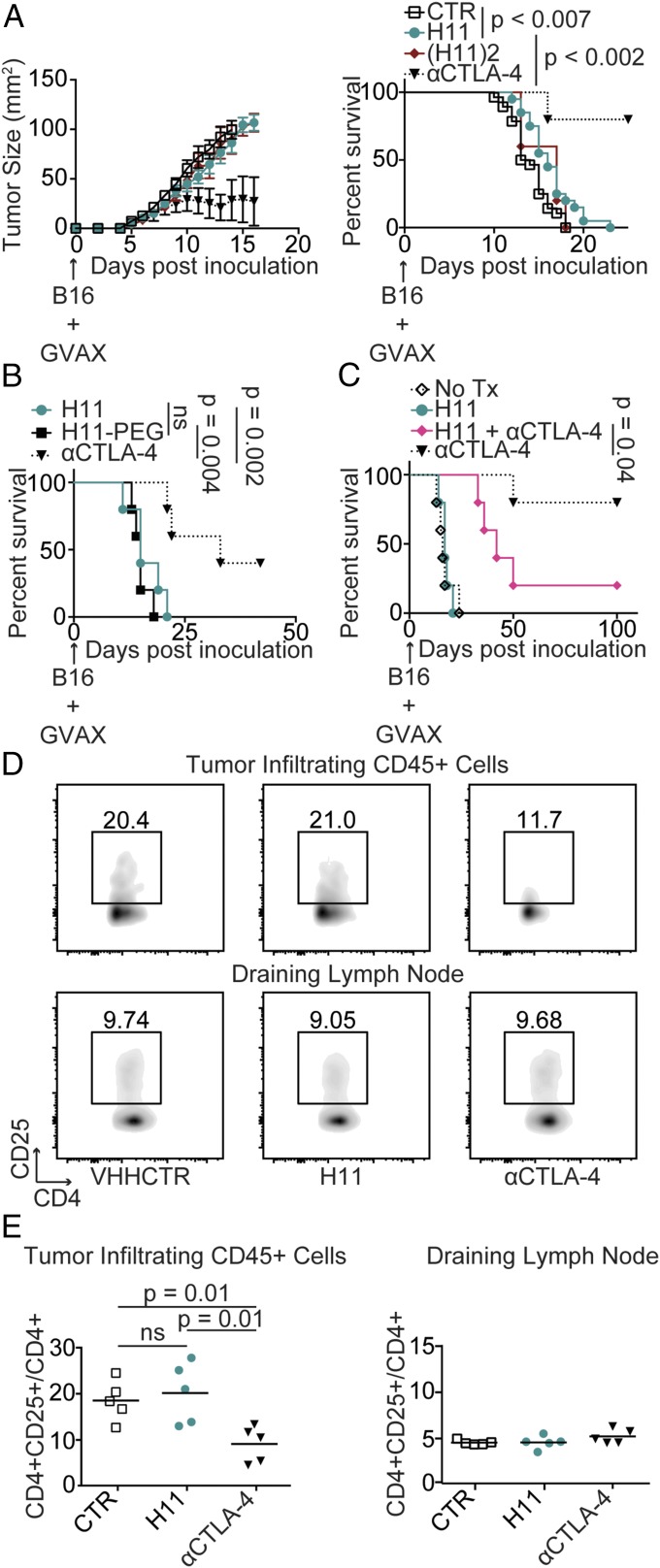
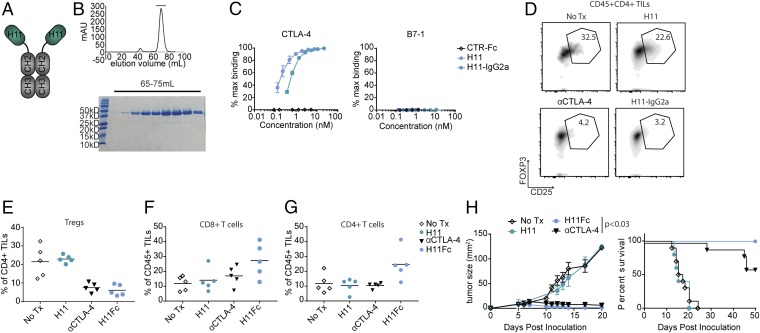
Ipilimumab, a monoclonal antibody that recognizes cytotoxic T lymphocyte antigen (CTLA)-4, was the first approved "checkpoint"-blocking anticancer therapy. In mouse tumor models, the response to antibodies against CTLA-4 depends entirely on expression of the Fcγ receptor (FcγR), which may facilitate antibody-dependent cellular phagocytosis, but the contribution of simple CTLA-4 blockade remains unknown. To understand the role of CTLA-4 blockade in the complete absence of Fc-dependent functions, we developed H11, a high-affinity alpaca heavy chain-only antibody fragment (VHH) against CTLA-4. The VHH H11 lacks an Fc portion, binds monovalently to CTLA-4, and inhibits interactions between CTLA-4 and its ligand by occluding the ligand-binding motif on CTLA-4 as shown crystallographically. We used H11 to visualize CTLA-4 expression in vivo using whole-animal immuno-PET, finding that surface-accessible CTLA-4 is largely confined to the tumor microenvironment. Despite this, H11-mediated CTLA-4 blockade has minimal effects on antitumor responses. Installation of the murine IgG2a constant region on H11 dramatically enhances its antitumor response. Coadministration of the monovalent H11 VHH blocks the efficacy of a full-sized therapeutic antibody. We were thus able to demonstrate that CTLA-4-binding antibodies require an Fc domain for antitumor effect.
Keywords: CTLA-4; cancer; checkpoint blockade; immunotherapy; single-domain antibody.
Copyright © 2018 the Author(s). Published by PNAS.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
