Osseous changes in the temporomandibular joint in rheumatoid arthritis: A cone-beam computed tomography study
- PMID: 29581944
- PMCID: PMC5863014
- DOI: 10.5624/isd.2018.48.1.1
Osseous changes in the temporomandibular joint in rheumatoid arthritis: A cone-beam computed tomography study
Abstract
Purpose: To evaluate osseous changes of temporomandibular joint (TMJ) in patients with rheumatoid arthritis (RA) using cone-beam computed tomography (CBCT) and to correlate the imaging findings with the severity of TMJ dysfunction, clinical findings, and laboratory findings.
Materials and methods: This study consisted of 28 subjects, including 14 RA patients and 14 controls, who were scheduled to undergo CBCT imaging for the diagnosis of a complaint not related to or affecting the TMJ. The Fonseca's questionnaire was used to assess the severity of TMJ dysfunction. Rheumatoid factor (RF) and the erythrocyte sedimentation rate (ESR) were assessed in the RA patients. CBCT was then performed in all subjects and osseous TMJ abnormalities were assessed.
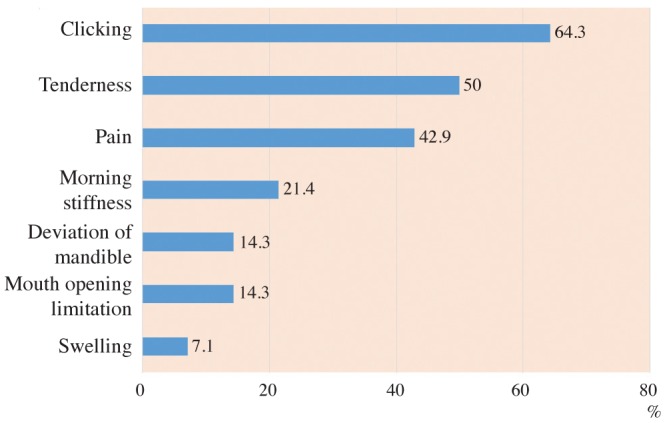
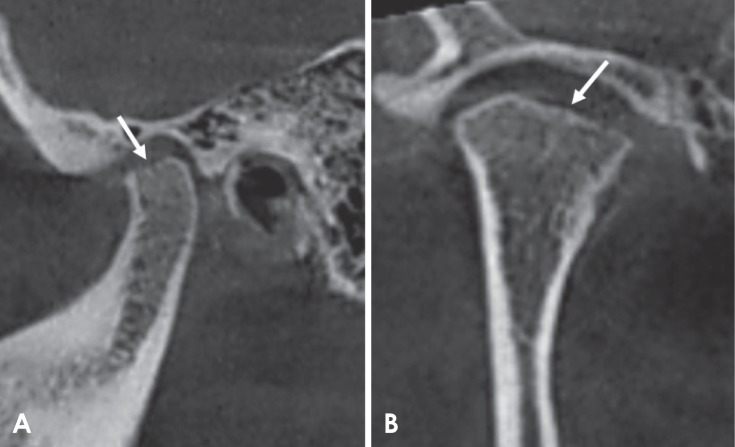
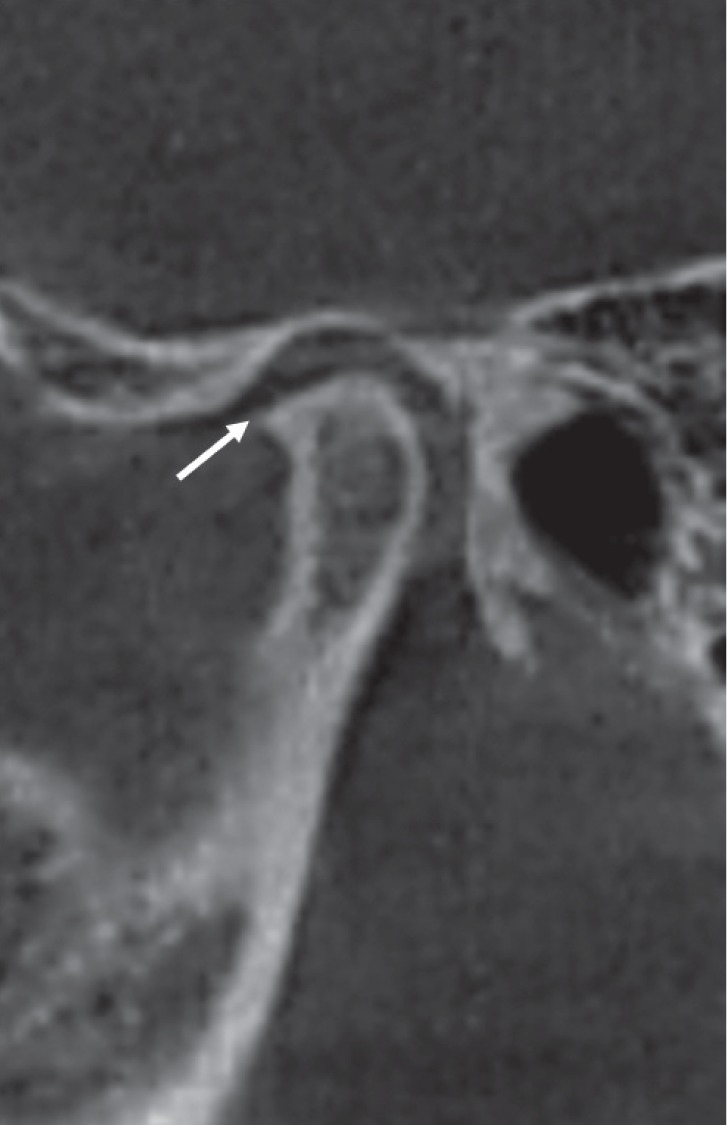
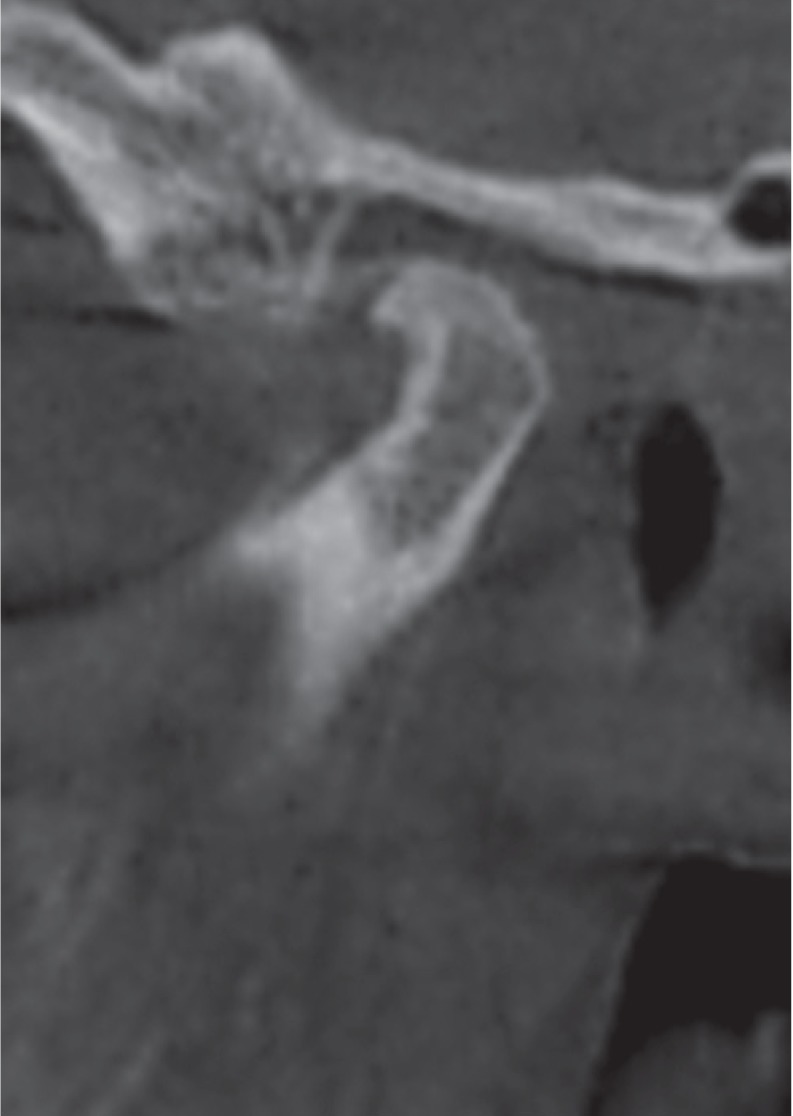
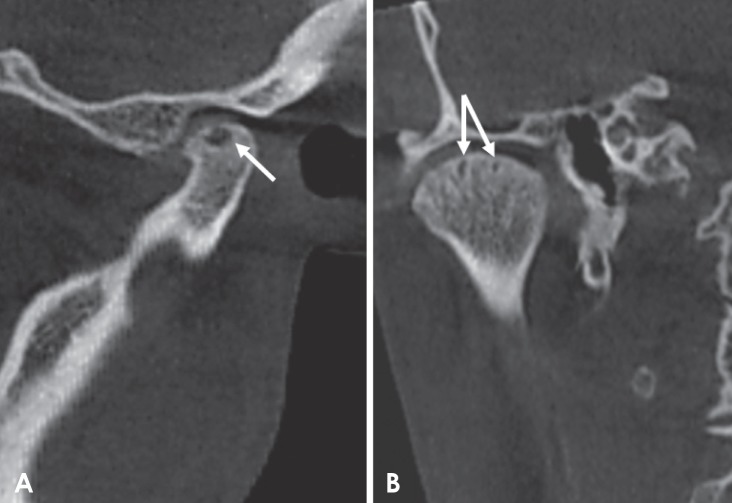
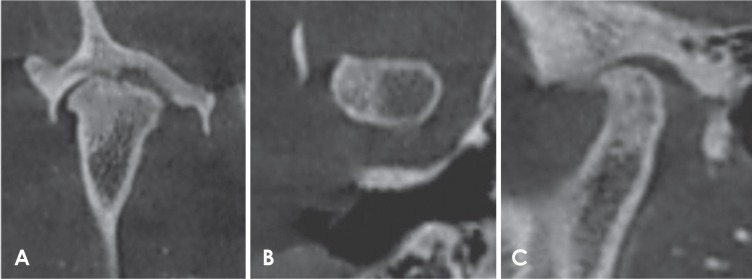
Results: According to the Fonseca's questionnaire, 14.3% of the patients had no TMJ dysfunction, while 50%, 21.4%, and 14.3% had mild, moderate, and severe dysfunction, respectively. RF was positive in 64.3% of patients, and the ESR level was high in 100%. Imaging findings revealed a statistically significantly higher prevalence of erosion (85.7%), flattening (89.3%), osteophyte formation (32.1%), subchondral cyst (32.1%), sclerosis (64.3%), and condylar irregularities (28.6%) in the RA patients than in the controls. No correlations were found between CBCT findings and the clinical findings, the severity of TMJ dysfunction, disease duration, or laboratory results.
Conclusion: RA patients might show extensive osseous abnormalities with no/mild clinical signs or symptoms of TMJ dysfunction that necessitate TMJ imaging for these patients. CBCT is a valuable and efficient modality that can assess osseous TMJ changes in RA patients.
Keywords: Arthritis, Rheumatoid; Cone-Beam Computed Tomography; Temporomandibular Joint.
Figures


References
-
- Yilmaz HH, Yildirim D, Ugan Y, Tunc SE, Yesildag A, Orhan H, et al. Clinical and magnetic resonance imaging findings of the temporomandibular joint and masticatory muscles in patients with rheumatoid arthritis. Rheumatol Int. 2012;32:1171–1178. - PubMed
-
- Rindfleisch JA, Muller D. Diagnosis and management of rheumatoid arthritis. Am Fam Physician. 2005;72:1037–1047. - PubMed
-
- American College of Rheumatology Subcommittee on Rheumatoid Arthritis Guidelines. Guidelines for the management of rheumatoid arthritis: 2002 Update. Arthritis Rheum. 2002;46:328–346. - PubMed
-
- Assasi N, Blackhouse G, Campbell K, Hopkins RB, Levine M, Richter T, et al. Comparative value of erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) testing in combination versus individually for the diagnosis of undifferentiated patients with suspected inflammatory disease or serious infection: a systematic review and economic analysis. Ottawa, ON: Canadian Agency for Drugs and Technologies in Health; 2015. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous