

Dual Antiplatelet Therapy in Transient Ischemic Attack and Minor Stroke With Different Infarction Patterns: Subgroup Analysis of the CHANCE Randomized Clinical Trial
- PMID: 29582084
- PMCID: PMC5885215
- DOI: 10.1001/jamaneurol.2018.0247
Dual Antiplatelet Therapy in Transient Ischemic Attack and Minor Stroke With Different Infarction Patterns: Subgroup Analysis of the CHANCE Randomized Clinical Trial
Abstract
Importance: Infarction patterns may serve as important imaging markers to assess the probability of stroke recurrence in transient ischemic attack (TIA) and minor stroke. However, it is unclear whether patients with different infarction patterns benefit differently from dual antiplatelet therapy.
Objectives: To investigate whether infarction patterns can stratify the risk of recurrent stroke and whether the efficacy and safety of clopidogrel plus aspirin vs aspirin alone are consistent in different infarction patterns after TIA or minor stroke.
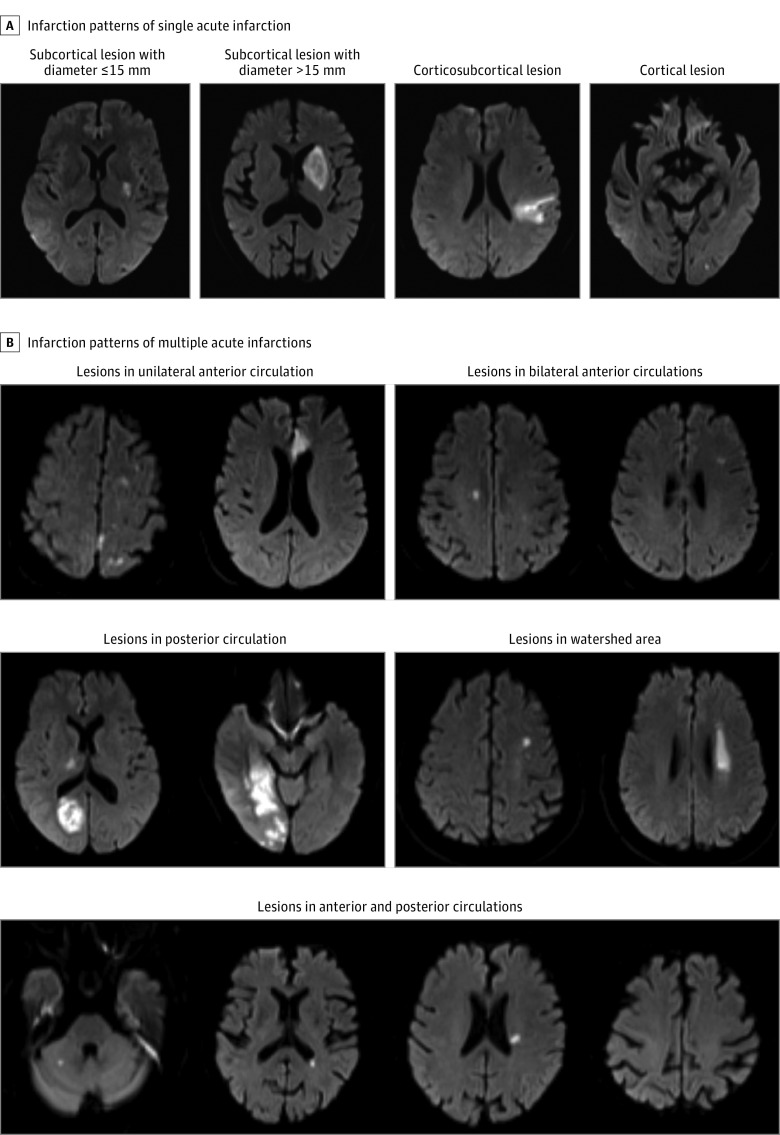
Design, setting, and participants: In this prespecified imaging substudy of the Clopidogrel in High-Risk Patients With Acute Nondisabling Cerebrovascular Events (CHANCE) randomized clinical trial, a total of 1342 patients with noncardioembolic TIA or minor stroke at 45 sites of CHANCE from October 1, 2009, to July 30, 2012, were included in this substudy. The final analysis was conducted on July 30, 2016, and included 1089 patients with required magnetic resonance imaging sequences. Infarction patterns were grouped into multiple acute infarctions (MAIs), single acute infarction (SAI), and no acute infarction (NAI) according to diffusion-weighted imaging.
Main outcomes and measures: Primary and secondary efficacy outcomes were stroke recurrence and new clinical vascular event after 3 months, respectively. The safety outcome was moderate to severe bleeding risk after 3 months.
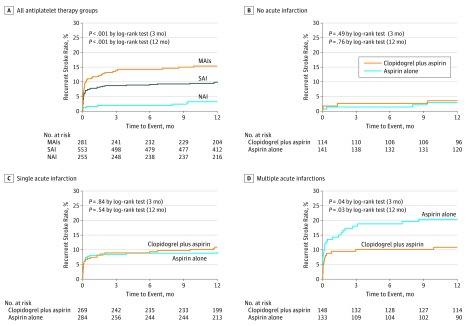
Results: Among 1089 patients, the mean (SD) age was 63.1 (10.7) years and 731 patients (65%) were men. Patients with MAIs (hazard ratio [HR], 5.8; 95% CI, 2.2-15.1; P < .001) and SAI (HR, 3.9; 95% CI, 1.5-10.5; P = .007) had higher risk of recurrent stroke than those with NAI after adjustment for potential confounders at 3-month follow-up. Stroke recurrence occurred in 15 (10.1%) and 25 (18.8%) of patients with MAIs administered clopidogrel plus aspirin and placebo plus aspirin, respectively (HR, 0.5; 95% CI, 0.3-0.96; P = .04), 24 (8.9%) and 24 (8.5%) of patients with SAI administered clopidogrel plus aspirin and placebo plus aspirin, respectively (HR, 1.1; 95% CI, 0.6-2.0; P = .71), and 3 (2.6%) and 2 (1.4%) of patients with NAI administered clopidogrel plus aspirin and placebo plus aspirin, respectively (HR, 1.7; 95% CI, 0.3-11.1; P = .56), with P = .04 for treatment × infarction pattern interaction effect. Clopidogrel plus aspirin did not increase moderate to severe bleeding risk.
Conclusions and relevance: Infarction patterns can efficiently stratify the risk of recurrent stroke within 3 months of noncardioembolic TIA or minor ischemic stroke. Patients with MAIs received the most pronounced clinical benefit from dual antiplatelet therapy without increasing the risk of moderate to severe bleeding. However, even if after dual antiplatelet treatment, patients with MAIs still had a risk of stroke recurrence as high as those with SAI.
Trial registration: clinicaltrials.gov Identifier: NCT00979589.
Conflict of interest statement
Figures
References
-
- von Weitzel-Mudersbach P, Andersen G, Hundborg HH, Johnsen SP. Transient ischemic attack and minor stroke are the most common manifestations of acute cerebrovascular disease: a prospective, population-based study—the Aarhus TIA study. Neuroepidemiology. 2013;40(1):50-55. - PubMed
-
- Wu CM, McLaughlin K, Lorenzetti DL, Hill MD, Manns BJ, Ghali WA. Early risk of stroke after transient ischemic attack: a systematic review and meta-analysis. Arch Intern Med. 2007;167(22):2417-2422. - PubMed
-
- Johnston SC, Gress DR, Browner WS, Sidney S. Short-term prognosis after emergency department diagnosis of TIA. JAMA. 2000;284(22):2901-2906. - PubMed
-
- Giles MF, Rothwell PM. Risk of stroke early after transient ischaemic attack: a systematic review and meta-analysis. Lancet Neurol. 2007;6(12):1063-1072. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
