

doi: 10.1111/jdi.12810.
Online ahead of print.
Japanese Clinical Practice Guideline for Diabetes 2016
Affiliations
- PMID: 29582574
- PMCID: PMC5934251
- DOI: 10.1111/jdi.12810
Item in Clipboard
Japanese Clinical Practice Guideline for Diabetes 2016
J Diabetes Investig.
.
Erratum in
-
Eratum.J Diabetes Investig. 2019 Jan;10(1):190. doi: 10.1111/jdi.12979. Epub 2018 Dec 3. J Diabetes Investig. 2019. PMID: 30609323 Free PMC article. No abstract available.
-
Corrigendum.J Diabetes Investig. 2020 May;11(3):752. doi: 10.1111/jdi.13252. J Diabetes Investig. 2020. PMID: 32419345 Free PMC article. No abstract available.
No abstract available
Keywords: Diabetes; Diagnosis; Guideline; Treatment.
Figures
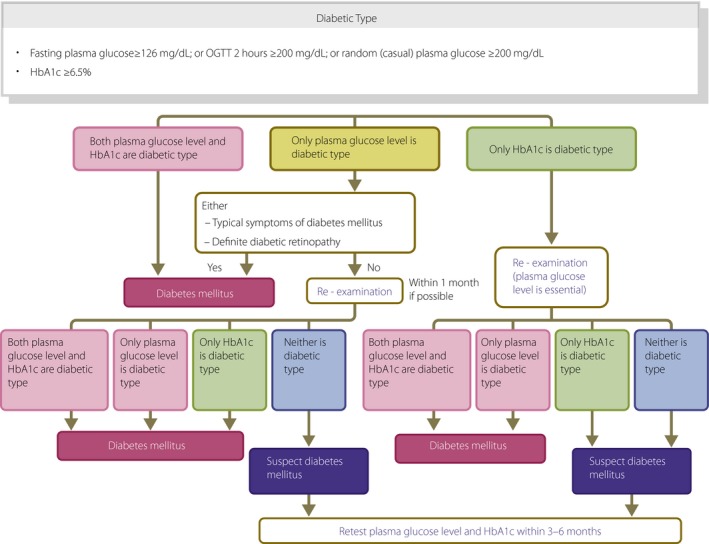
Flow chart outlining the steps in the clinical diagnosis of diabetes mellitus. OGTT , Oral glucose tolerance test.
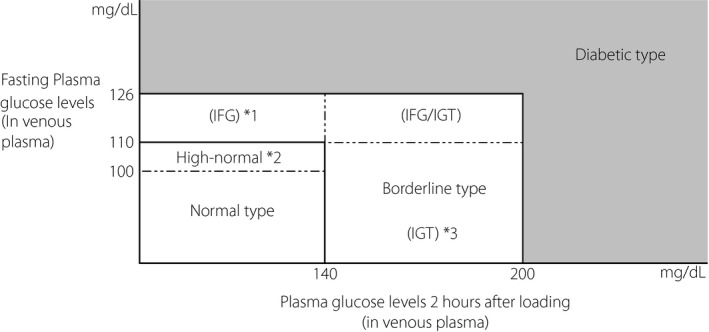
The categories of glycemia as indicated by fasting plasma glucose levels and 75 g OGTT results. *1 The impaired fasting glucose (IFG ) category represents cases of fasting plasma glucose levels of 110–125 mg/dL (6.1–7.0 mmol/L) and 2‐h plasma glucose levels of <140 mg/dL (7.8 mmol/L) in a 75 g OGTT (WHO ). However, in the ADA criteria, IFG is defined as a fasting plasma glucose levels of 100–125 mg/dL (5.6–7.0 mmol/L), and only FPG is used for the determination of IFG . *2 Fasting plasma glucose levels of 100–109 mg/dL (5.6–6.1 mmol/L) are within the normal limits, but are considered to be ‘high‐normal’. Because patients with a high‐normal glucose level are at risk of developing diabetes and include cases with various degrees of impaired glucose tolerance, the performance of an OGTT is desirable. *3 The category was adopted by the WHO in the diagnostic criteria for diabetes mellitus, and represents cases with fasting plasma glucose levels of <126 mg/dL and 2‐h plasma glucose levels of 140–199 mg/dL (7.8–11.1 mmol/L in a 75 g OGTT .
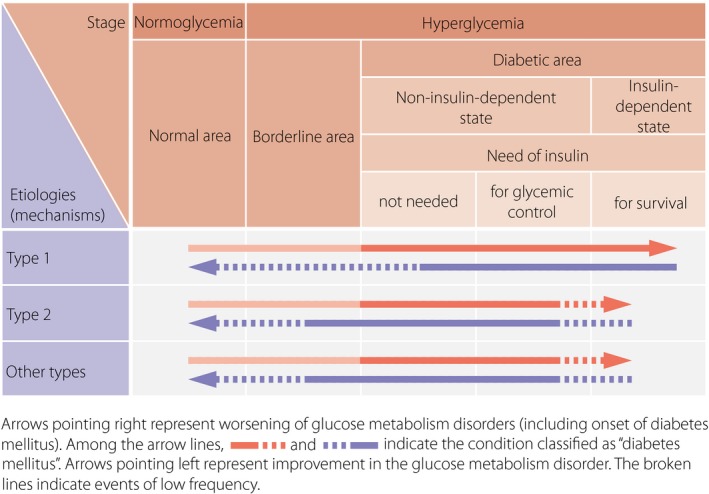
A schematic diagram of the relationship between the etiology (mechanism) and pathophysiological stages (states) of diabetes mellitus. Arrows pointing right represent the worsening of glucose metabolism disorders (including the onset of diabetes mellitus). Among the arrow lines, indicates the condition classified as ‘diabetes mellitus’. Arrows pointing left represent improvement in the glucose metabolism disorder. The broken lines indicate events of low frequency. For example, in type 2 diabetes mellitus, infection can lead to ketoacidosis and require temporary insulin treatment for survival. Also, once diabetes mellitus has developed, it is treated as diabetes mellitus regardless of the improvement in the glucose metabolism; thus, the arrow lines pointing left are filled in black. In such cases, a broken line is used, because complete normalization of the glucose metabolism is rare.
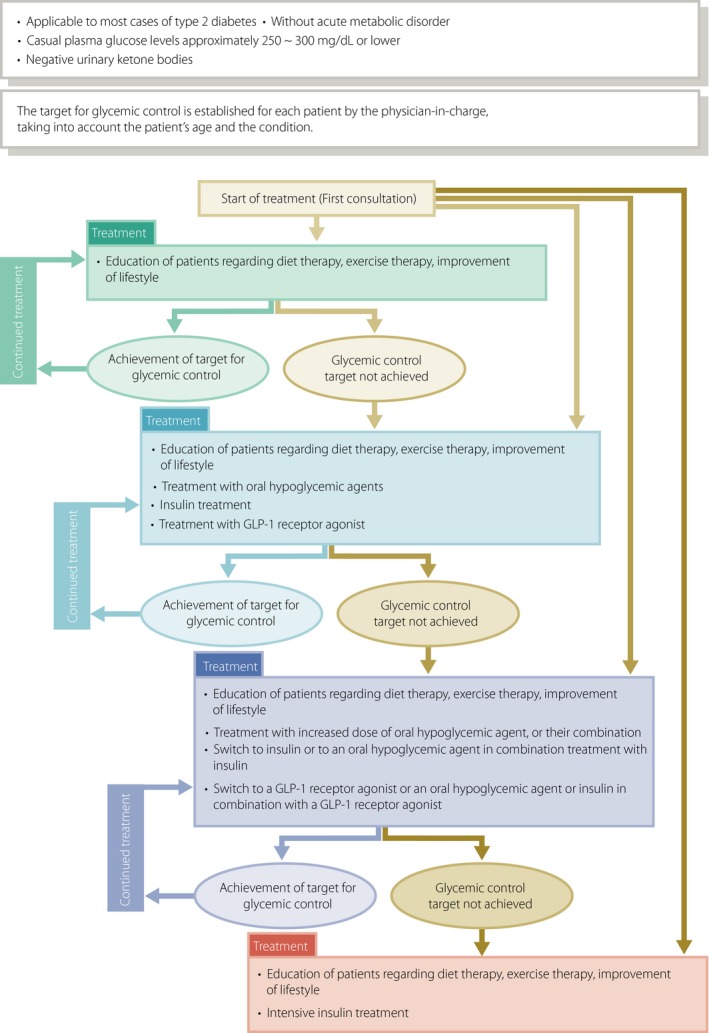
Treatment of patients in a non‐insulin‐dependent state. This provides a guide to the management of patients without acute metabolic disorder (i.e., those who had a casual blood glucose level of 250–300 mg/dL [13.9–16.7 mmol/L] or less than 250 to 300 mg/dL with a negative urinary ketone test). The glycemic goal should be determined individually depending on the disease condition or age of the patient but is generally set at HbA1c <7.0%. ‘Diet therapy’ and ‘exercise therapy’ are referred to as ‘medical nutrition therapy (MNT )’ and ‘physical activity/exercise’, respectively, elsewhere in this guideline.
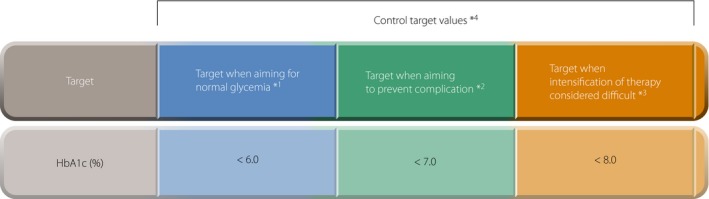
Glycemic control targets. Control targets are established individually, in consideration of age, duration of disease, organ damage, risk of hypoglycemia, support structures, etc. *1 When targets can be attained by appropriate MNT or physical activity/exercise, or during pharmacotherapy without the occurrence of side effects such as hypoglycemia. *2 From the perspective of preventing complication, HbA1c target value is set at <7%. A fasting blood glucose level <130 mg/dL (7.2 mmol/L) and a 2‐h postprandial blood glucose level <180 mg/dL (10.0 mmol/L) can be used as an approximate guideline for the corresponding blood glucose levels. *3 When intensification of treatment is considered difficult due to side effects such as hypoglycemia or for other reasons. *4 All target values are for adults, not including pregnant women.
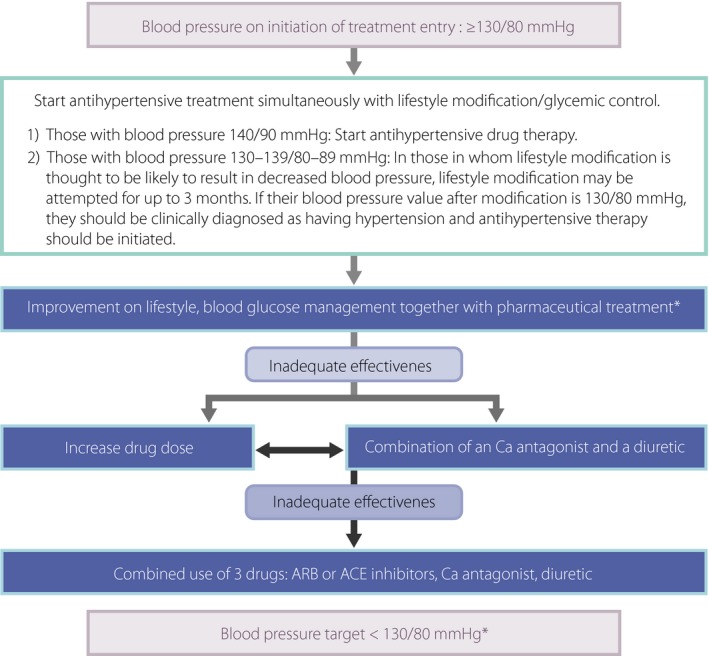
The treatment of hypertension complicating diabetes mellitus. Excerpt from: The Japanese Society of Hypertension, Guidelines for the Treatment of Hypertension, 2014, p. 78. *Care needs to be taken to closely monitor patients with coronary atherosclerosis, peripheral arterial disease, or older patients with diabetes, for decreased organ blood flow.
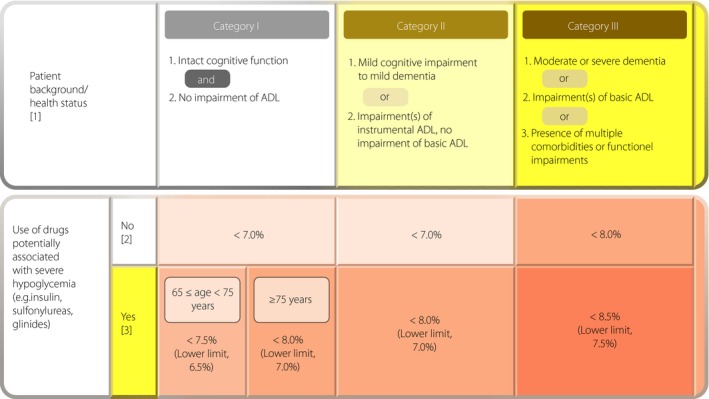
Glycemic targets (HbA1c values) for older patients with diabetes. For older patients, the glycemic target is to be determined for each patient by taking into account his/her age, duration of diabetes, risk of hypoglycemia, and any support available to the patient, as well as the patient's cognitive function, basic/instrumental activities of daily living (ADL), and comorbidities/functional impairments, while noting the potential risk of hypoglycemia that increases with age in each patient. (1) Refer to the Japan Geriatrics Society website1, 2, for the evaluation of the cognitive function, basic ADL (e.g., self‐care abilities such as dressing, transferring, bathing, and toileting), and instrumental ADL (e.g., the patient's ability to maintain an independent household by performing activities such as shopping, meal preparation, taking medication, and handling finances). In end‐of‐life care, priority is to be given to preventing significant hyperglycemia and subsequent dehydration and acute complications through appropriate therapeutic measures. (2) As in other age groups, the glycemic target for preventing diabetic complications in older patients with diabetes is set to <7.0%. However, this can be set to <6.0% for those who are thought to be likely to achieve glycemic control through MNT and/or physical activity/exercise alone or those who are likely to achieve glycemic control with drug therapy without adverse reactions, or 8.0% for those in whom intensifying therapy may prove difficult. In either case, no lower limit is specified for the glycemic target. A glycemic target of <8.5% may be allowed in patients who are thought to be in category III and therefore at risk of developing adverse reactions to multi‐drug combination therapy or in those with serious comorbidities or poor social support. (3) In patients in whom priority should be given to preventing the onset/progression of diabetic complications due to their duration of disease, the glycemic target or its lower limit may be set for each older patient with appropriate measures in place to prevent severe hypoglycemia. Current treatments are to be continued in those who are <65 years of age, even when their HbA1c values fall below their glycemic target or a lower limit while on therapy; however, care needs to be taken to monitor these patients for potential severe hypoglycemia. Glinides may be classified as drugs that are unlikely to be associated with severe hypoglycemia, as the onset of severe hypoglycemia varies depending on the type and amount of glinide used in a particular patient relative to the patient's glucose level.
Similar articles
-
[Comparison between guideline for diagnosis procedure combination by Japanese Society of Laboratory Medicine in 2003 and clinical pass of Yamagata University Hospital].Rinsho Byori. 2004 Dec;52(12):991-5. Rinsho Byori. 2004. PMID: 15675346 Japanese.
-
Clinical practice guidelines for gastrointestinal stromal tumor (GIST) in Japan: English version.Int J Clin Oncol. 2008 Oct;13(5):416-30. doi: 10.1007/s10147-008-0798-7. Epub 2008 Oct 23. Int J Clin Oncol. 2008. PMID: 18946752
-
Diagnosis and treatment of bone metastasis: comprehensive guideline of the Japanese Society of Medical Oncology, Japanese Orthopedic Association, Japanese Urological Association, and Japanese Society for Radiation Oncology.ESMO Open. 2016 Mar 16;1(2):e000037. doi: 10.1136/esmoopen-2016-000037. eCollection 2016. ESMO Open. 2016. PMID: 27843593 Free PMC article. Review.
-
Japanese Clinical Practice Guideline for Diabetes 2016.Diabetol Int. 2018 Mar 27;9(1):1-45. doi: 10.1007/s13340-018-0345-3. eCollection 2018 Feb. Diabetol Int. 2018. PMID: 30603347 Free PMC article. Review. No abstract available.
-
Japanese Clinical Practice Guideline for Diabetes 2019.Diabetol Int. 2020 Jul 24;11(3):165-223. doi: 10.1007/s13340-020-00439-5. eCollection 2020 Jul. Diabetol Int. 2020. PMID: 32802702 Free PMC article. Review. No abstract available.
Cited by
-
Associations between physical frailty and living arrangements in Japanese older adults living in a rural remote island: The Shimane CoHRE study.J Gen Fam Med. 2022 Apr 10;23(5):310-318. doi: 10.1002/jgf2.544. eCollection 2022 Sep. J Gen Fam Med. 2022. PMID: 36093222 Free PMC article.
-
Multiple daily insulin injections ameliorate QT interval by lowering blood glucose levels in patients with type 2 diabetes.Ther Adv Endocrinol Metab. 2021 Apr 22;12:20420188211010057. doi: 10.1177/20420188211010057. eCollection 2021. Ther Adv Endocrinol Metab. 2021. PMID: 34104393 Free PMC article.
-
Diabetes Monotherapies versus Metformin-Based Combination Therapy for the Treatment of Type 2 Diabetes.Int J Gen Med. 2021 Jul 24;14:3833-3848. doi: 10.2147/IJGM.S295459. eCollection 2021. Int J Gen Med. 2021. PMID: 34335049 Free PMC article. Review.
-
Association between mandatory health examination attendance and diabetes treatment initiation among employees being treated for hypertension.J Occup Health. 2020 Jan;62(1):e12183. doi: 10.1002/1348-9585.12183. J Occup Health. 2020. PMID: 33296133 Free PMC article.
-
A randomized controlled trial of two diets enriched with protein or fat in patients with type 2 diabetes treated with dapagliflozin.Sci Rep. 2021 May 31;11(1):11350. doi: 10.1038/s41598-021-90879-z. Sci Rep. 2021. PMID: 34059720 Free PMC article. Clinical Trial.
References
1 Guideline for the diagnosis of diabetes mellitus
-
- Kosaka K, Akanuma Y, Goto Y, et al Report of committee on the classification and diagnostic criteria of diabetes mellitus. J Jpn Diabetes Soc 1982; 25: 859–866 (in Japanese).
-
- The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus . Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 1997; 20: 1183–1197. - PubMed
-
- World Health Organization . Report of a WHO Consultation: Definition, Diagnosis and Classification of Diabetes Mellitus and its Complications. Part 1: Diagnosis and Classification of Diabetes Mellitus. Geneva: World Health Organization Department of Noncommunicable Disease Surveillance, 1999. Available from: http://www.staff.ncl.ac.uk/philip.home/who_dmc.htm
-
- Kuzuya T, Nakagawa S, Satoh J, et al Report of the committee of Japan Diabetes Society on the classification and diagnostic criteria of diabetes mellitus. J Jpn Diabetes Soc 1999; 42: 385–404 (in Japanese).
2 Goals and strategies for diabetes management
-
- United Kingdom Prospective Diabetes Study (UKPDS) Group . Intensive blood‐glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS33). Lancet 1998; 352: 837–853 (level 1+). - PubMed
-
- Sone H, Tanaka S, Tanaka S, et al Serum level of triglycerides is a potent risk factor comparable to LDL cholesterol for coronary heart disease in Japanese patients with type 2 diabetes: subanaysis of the Japan Diabetes Complications Study (JDCS). J Clin Endocrinol Metab 2011; 96: 3448–3456 (level 2). - PubMed
3 Medical nutrition therapy (MNT)
-
- Nakagawa Y, Ishikawa Y, Watanabe K, et al Impact of the duration of diabetes and frequency of counseling on the effectiveness of dietitian‐led medical nutrition therapy in patients with type 2 diabetes. J Jpn Diabetes Soc 2014; 57: 813–819 (in Japanese) (level 3).
-
- Pastors JG, Warshaw H, Daly A, et al The evidence for the effectiveness of medical nutrition therapy in diabetes management. Diabetes Care 2002; 25: 608–613 (level 3). - PubMed
4 Physical activity/exercise
-
- American Diabetes Association . Foundations of care and comprehensive medical evaluation. Sec. 3. In Standards of Medical Care in Diabetes‐2016. Diabetes Care 2016; 39 (Suppl. 1) : S23–S35. - PubMed
-
- Marwick TH, Hordern MD, Miller T, et al Exercise training for type 2 diabetes mellitus: impact on cardiovascular risk: a scientific statement from the American Heart Association. Circulation 2009; 119: 3244–3262. - PubMed
-
- Umpierre D, Ribeiro PA, Kramer CK, et al Physical activity advice only or structured exercise training and association with HbA1c levels in type 2 diabetes: a systematic review and meta‐analysis. JAMA 2011; 305: 1790–1799 (level 1). - PubMed
-
- Boulé NG, Kenny GP, Haddad E, et al Meta‐analysis of the effect of structured exercise training on cardiorespiratory fitness in type 2 diabetes mellitus. Diabetologia 2003; 46: 1071–1081 (level 1). - PubMed
5 Treatment with glucose‐lowering agents (excluding insulin)
-
- UK Prospective Diabetes Study (UKPDS) Group . Intensive blood‐glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998; 352: 837–853 (level 1+). - PubMed
-
- Inzucchi SE, Bergenstal RM, Buse JB, et al Management of hyperglycemia in type 2 diabetes, 2015: a patient‐centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2015; 381: 140–149. - PubMed
-
- UK Prospective Diabetes Study (UKPDS) Group . Effect of intensive blood‐glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998; 352: 854–865 (level 1+). - PubMed
6 Insulin therapy
-
- The Diabetes Control and Complications Trial (DCCT) Research Group . Early worsening of diabetic retinopathy in the Diabetes Control and Complications Trial. Arch Ophthalmol 1998; 116: 874–886 (level 1+). - PubMed
-
- Takahashi Y, Takayama S, Ito T, et al Clinical features of eighty‐six diabetic patients with post‐treatment painful neuropathy. J Jpn Diabetes Soc 1998; 41: 165–170 (in Japanese) (level 4).
-
- United Kingdom Prospective Diabetes Study (UKPDS) Group . United Kingdom Prospective Diabetes Study 24: a 6‐year, randomized, controlled trial comparing sulfonylurea, insulin, and metformin therapy in patients with newly diagnosed type 2 diabetes that could not be controlled with diet therapy. Ann Intern Med 1998; 128: 165–175 (level 1). - PubMed
-
- The Diabetes Control and Complications Trial (DCCT) Research Group . The effect of intensive treatment of diabetes on the development and progression of long‐term complications in insulin‐dependent diabetes mellitus. N Engl J Med 1993; 329: 977–986 (level 1+). - PubMed
7 Diabetes self management education and support and education for the self management of diabetes
-
- Tshiananga JK, Kocher S, Weber C, et al The effect of nurse‐led diabetes self‐management education on glycosylated hemoglobin and cardiovascular risk factors: a meta‐analysis. Diabetes Educ 2012; 38: 108–123 (level 1). - PubMed
-
- Minet L, Moller S, Vach W, et al Mediating the effect of self‐care management intervention in type 2 diabetes: a meta‐analysis of 47 randomised controlled trials. Patient Educ Couns 2010; 80: 29–41 (level 1). - PubMed
-
- Deakin T, McShane CE, Cade JE. Group based training for self‐management strategies in people with type 2 diabetes mellitus. Cochrane Database Syst Rev 2005: CD003417 (level 1). - PubMed
-
- The Diabetes Control and Complications Trial Research Group . The effect of intensive treatment of diabetes on the development and progression of long‐term complications in insulin‐dependent diabetes mellitus. N Engl J Med 1993; 329: 977–986 (level 1). - PubMed
8 Diabetic retinopathy
-
- Klein R, Klein BE, Moss SE, et al The Wisconsin Epidemiologic Study of Diabetic Retinopathy: IX. Four year incidence and progression of diabetic retinopathy when age at diagnosis is less than 30 years. Arch Ophthalmol 1989; 107: 237–243 (level 2). - PubMed
-
- Klein R, Klein BE, Moss SE, et al The Wisconsin Epidemiologic Study of Diabetic Retinopathy: X. Four year incidence and progression of diabetic retinopathy when age at diagnosis is 30 years or more. Arch Ophthalmol 1989; 107: 244–249 (level 2). - PubMed
-
- Younis N, Broadbent DM, Vora JP, et al Incidence of sight‐threatening retinopathy in patients with type 2 diabetes in the Liverpool Diabetic Eye Study: a cohort study. Lancet 2003; 361: 195–200 (level 2). - PubMed
-
- Misra A, Bachmann MO, Greenwood RH, et al Trends in yield and effects of screening intervals during 17 years of a large UK community‐based diabetic retinopathy screening programme. Diabet Med 2009; 26: 1040–1047 (level 2). - PubMed
-
- Diabetes Control and Complications Trial Research Group . The effect of intensive treatment of diabetes on the development and progression of long‐term complications in insulin‐dependent diabetes mellitus. N Engl J Med 1993; 329: 977–986 (level 1+). - PubMed
9 Diabetic nephropathy
-
- Matsuo S, Imai E, Horio M, et al Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis 2009; 5: 982–992. - PubMed
-
- Horio M, Imai E, Yasuda Y; Collaborators Developing the Japanese Equation for Estimated GFR . GFR estimation using standardized serum cystatin C in Japan. Am J Kidney Dis 2013; 61: 197–203. - PubMed
-
- Ohkubo Y, Kishikawa H, Araki E, et al Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non‐insulin‐dependent diabetes mellitus: a randomized prospective 6‐year study. Diabetes Res Clin Pract 1995; 28: 103–117 (level 1). - PubMed
-
- Patel A, MacMahon S, Chalmers J, et al Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 2008; 358: 2560–2572 (level 1+). - PubMed
10 Diabetic neuropathy
-
- Hotta N, Toyoda R. Diabetic Neuropathy 1996; 145–154. Kanehara, Tokyo (in Japanese).
-
- Boulton AJ, Vinik AI, Arezzo JC, et al Diabetic neuropathies: a statement by the American DiabetesAssociation. Diabetes Care 2005; 28: 956–962. - PubMed
-
- Tesfaye S, Chaturvedi N, Eaton SE, et al Vascular risk factors and diabetic neuropathy. N Engl J Med 2005; 352: 341–350 (level 2). - PubMed
-
- The Diabetes Control and Complications Trial (DCCT) Research Group . The effect of intensive treatment of diabetes on the development and progression of long‐term complications in insulin‐dependent diabetes mellitus. N Engl J Med 1993; 329: 977–986 (level 1+). - PubMed
-
- Ohkubo Y, Kishikawa H, Araki E, et al Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non‐insulin‐dependent diabetes mellitus: a randomized prospective 6‐year study. Diabetes Res Clin Pract 1995; 28: 103–117 (level 1). - PubMed
11 Diabetic foot
-
- International Working Group on the Diabetic Foot (IWGDF) . Guidance, 2015. Available from: http://iwgdf.org/guidelines-2/
-
- Frykberg RG, Zgonis T, Armstrong DG, et al Diabetic foot disorders: a clinical practice guideline (2006 revision). J Foot Ankle Surg 2006; 45: S1–S66. - PubMed
-
- Krishinan S, Nash F, Baker N, et al Reduction in diabetic amputations over 11 years in a defined U.K. population: benefits of multidisciplinary team work and continuous prospective audit. Diabetes Care 2008; 31: 99–101 (level 2). - PubMed
-
- Malone JM, Snyder M, Anderson G, et al Prevention of amputation by diabetic education. Am J Surg 1989; 158: 520–524 (level 1). - PubMed
12 Diabetic macroangiopathy
-
- Gaede P, Vedel P, Larsen N, et al Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N Engl J Med 2003; 348: 383–393 (level 1). - PubMed
13 Diabetes and periodontitis
-
- Takahashi K, Nishimura F, Kurihara M, et al Subgingival microflora and antibody responses against periodontal bacteria of young Japanese patients with type 1 diabetes mellitus. J Int Acad Periodontol 2001; 3: 104–111 (level 3). - PubMed
-
- Morita I, Inagaki K, Nakamura F, et al Relationship between periodontal status and levels of glycated hemoglobin. J Dent Res 2012; 91: 161–166 (level 3). - PubMed
-
- Borgnakke WS, Ylöstalo PV, Taylor GW, et al Effect of periodontal disease on diabetes: systematic review of epidemiologic observational evidence. J Periodontol 2013; 84: S135–S152 (level 2). - PubMed
14 Diabetes complicated by obesity (including metabolic syndrome)
-
- Matsuzawa Y, Sakata T, Ikeda Y, et al Guidelines for the management of obesity disease 2006. Obesity Research 2006; 12: 1–91 (in Japanese).
-
- Saito Y, Shirai A, Nakamura M, et al Diagnostic criteria for obesity disease 2011. Obesity Research 2011; 17: 1–78 (in Japanese).
-
- Van Gaal L, Scheen A. Weight management in type 2 diabetes: current and emerging approaches to treatment. Diabetes Care 2015; 38: 1161–1172. - PubMed
-
- Madigan CD, Aveyard P, Jolly K, et al Regular self‐weighing to promote weight maintenance after intentional weight loss: a quasi‐randomized controlled trail. J Public Health (Oxf) 2014; 36: 259–267 (level 2). - PubMed
15 Hypertension associated with diabetes
-
- Kengne AP, Patel A, Barzi F, et al Systolic blood pressure, diabetes and the risk of cardiovascular diseases in the Asia‐Pacific region. J Hypertens 2007; 25: 205–213 (level 2). - PubMed
-
- Patel A, MacMahon S, Chalmers J, et al Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet 2007; 370: 829–840 (level 1+). - PubMed
-
- American Diabetes Association . Microvascular complications and foot care: standards of medical care in diabetes 2016. Diabetes Care 2016; 39: S72–S80. - PubMed
-
- Bangalore S, Kumar S, Lobach I, et al Blood pressure targets in subjects with type 2 diabetes mellitus/impaired fasting glucose: observations from traditional and bayesian random‐effects metaanalysesof randomized trials. Circulation 2011; 123: 2799–2810 (level 1). - PubMed
16 Dyslipidemia associated with diabetes
-
- Sacks FM, Hermans MP, Fioretto P, et al Association between plasma triglycerides and high‐density lipoprotein cholesterol and microvascular kidney disease and retinopathy in type 2 diabetes mellitus: a global case–control study in 13 countries. Circulation 2014; 129: 999–1008 (level 3). - PubMed
-
- Heilbronn LK, Noakes M, Clifton PM. Effect of energy restriction, weight loss, and diet composition on plasma lipids and glucose in patients with type 2 diabetes. Diabetes Care 1999; 22: 889–895 (level 1). - PubMed
17 Impaired glucose metabolism in pregnancy
-
- Ray JG, O'Brien TE, Chan WS. Preconception care and the risk of congenital anomalies in the offspring of women with diabetes mellitus: a meta‐analysis. QJM 2001; 94: 435–444 (level 2). - PubMed
-
- Falavigna M, Schmidt MI, Trujillo J, et al Effectiveness of gestational diabetes treatment: a systematic review with quality of evidence assessment. Diabetes Res Clin Pract 2012; 98: 396–405 (level 2). - PubMed
-
- Metzger BE, Lowe LP, Dyer AR, et al Hyperglycemia and adverse pregnancy outcomes. N Engl J Med 2008; 358: 1991–2002 (level 2). - PubMed
-
- Ekbom P, Damm P, Feldt‐Rasmussen B, et al Pregnancy outcome in type 1 diabetic women with microalbuminuria. Diabetes Care 2001; 24: 1739–1744 (level 2). - PubMed
-
- Chew EY, Mills JL, Metzger BE, et al Metabolic control and progression of retinopathy: the Diabetes in Early Pregnancy Study. National Institute of Child Health and Human Development Diabetes in Early Pregnancy Study. Diabetes Care 1995; 18: 631–637 (level 2). - PubMed
18 Pediatric/adolescent diabetes
-
- ISPAD Clinical Practice Consensus Guidelines for Pediatric and Adolescent Diabetes 2014. Tokyo: Nankodo, 2015.
-
- Ascerini C, Craig ME, de Beaufort C, et al ISPAD clinical practice consensus guidelines 2014 compendium Introduction. Pediatr Diabetes 2014; 15(Suppl 20): 1–3. - PubMed
-
- Craig ME, Jefferies C, Dabelea D, et al ISPAD clinical practice consensus guidelines 2014 compendium. Definition, epidemiology, and classification of diabetes in children and adlescents. Pediatr Diabetes 2014; 15(Suppl 20): 4–17. - PubMed
-
- Ly TT, Maahs DM, Rewers A, et al ISPAD clinical practice consensus guidelines 2014 compendium. Assessment and management of hypoglycemia in children and adolescents with diabetes. Pediatr Diabetes 2014; 15(Suppl 20): 180–192. - PubMed
-
- Zeitler P, Fu J, Tandon N, et al ISPAD clinical practice consensus guidelines 2014 compendium Type 2 diabetes in the child and adolescent. Pediatr Diabetes 2014; 15(Suppl 20): 26–46. - PubMed
19 Diabetes in older adults
-
- Hideki Ito . Study to establish a treatment guideline for the elderly patients with diabetes mellitus, Research Reports of the Longevity Sciences volume 3, the Ministry of Health and Welfare of Japan. 1996; 309–311 (in Japanese) (level 3).
-
- Kuusisto J, Mykkänen L, Pyörälä K, et al NIDDM and its metabolic control predict coronary heart disease in elderly subjects. Diabetes 1994; 43: 960–967 (level 2). - PubMed
-
- Cukierman T, Gerstein HC, Williamson JD. Cognitive decline and dementia in diabetes‐systematic overview of prospective observational studies. Diabetologia 2005; 48: 2460–2469 (level 2). - PubMed
20 Acute metabolic complications of diabetes, sick days, and infectious diseases
-
- Nyenwe EA, Kitabchi AE. Evidence‐based management of hyperglycemic emergencies in diabetes mellitus. Diabetes Res Clin Pract 2011; 94: 340–351. - PubMed
-
- Wolfsdorf J, Glaser N, Sperling MA. Diabetic ketoacidosis in infants, children, and adolescents. Diabetes Care 2006; 29: 1150–1159. - PubMed
-
- Jeffrey A, Kraut MD, Nicolaos E, et al Lactic acidosis. N Engl J Med 2014; 371: 2309–2319. - PubMed
-
- Eppenga WL, Lalmohamed A, Geerts AF, et al Risk of lactic acidosis or elevated lactate concentrations in metformin users with renal impairment: a population‐based cohort study. Diabetes Care 2014; 37: 2218–2224 (level 2). - PubMed
21 Prevention of type 2 diabetes
-
- Heianza Y, Arase Y, Hsieh SD, et al Development of a new scoring system for predicting the 5 year incidence of type 2 diabetes in Japan: the Toranomon Hospital Health Management Center Study 6 (TOPICS 6). Diabetologia 2012; 55: 3213–3223 (level 3). - PubMed
-
- Sasai H, Sairenchi T, Irie F, et al [Development of a diabetes risk prediction sheet for specific health guidance]. Nihon Koshu Eisei Zasshi 2008; 55: 287–294 (in Japanese) (level 3). - PubMed
-
- Doi Y, Ninomiya T, Hata J, et al Two risk score models for predicting incident Type 2 diabetes in Japan. Diabet Med 2012; 29: 107–114 (level 2). - PubMed
-
- Kodama S, Horikawa C, Fujihara K, et al Comparisons of the strength of associations with future type 2 diabetes risk among anthropometric obesity indicators, including waist‐to‐height ratio: a meta‐analysis. Am J Epidemiol 2012; 176: 959–969 (level 2). - PubMed
-
- Kodama S, Horikawa C, Yoshizawa S, et al Body weight change and type 2 diabetes. Epidemiology 2013; 24: 778–779 (level 2). - PubMed
References for the appendix
-
- Bonovas S, Filioussi K, Tsantes A. Diabetes mellitus and risk of prostate cancer: a meta‐analysis. Diabetologia 2004; 47: 1071–1078. - PubMed
-
- Friberg E, Orsini N, Mantzoros CS, et al Diabetes mellitus and risk of endometrial cancer: a meta‐analysis. Diabetologia 2007; 50: 1365–1374. - PubMed
-
- Kasper JS, Giovannucci E. A meta‐analysis of diabetes mellitus and the risk of prostate cancer. Cancer Epidemiol Biomarkers Prev 2006; 15: 2056–2062. - PubMed
-
- Larsson SC, Orsini N, Wolk A. Diabetes mellitus and risk of colorectal cancer: a meta‐analysis. J Natl Cancer Inst 2005; 97: 1679–1687. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
