

Regional differences in aortic valve replacements: Atlantic Canadian experience
- PMID: 29582745
- PMCID: PMC5866144
- DOI: 10.1503/cjs.009517
Regional differences in aortic valve replacements: Atlantic Canadian experience
Abstract
Background: Transcatheter aortic valve implantation (TAVI) is evolving rapidly and is increasingly being adopted in the treatment of aortic valve disease. The goal of this study was to examine regional differences in surgical aortic valve replacement (SAVR) and TAVI across Atlantic Canada.
Methods: We identified all patients who underwent SAVR or TAVI between Jan. 1, 2010, and Dec. 31, 2014, in New Brunswick, Nova Scotia and Newfoundland and Labrador. Data obtained included patient demographic characteristics and surgical procedure details. We performed univariate descriptive analyses and calculated crude and age- and sex-adjusted incidence rates.
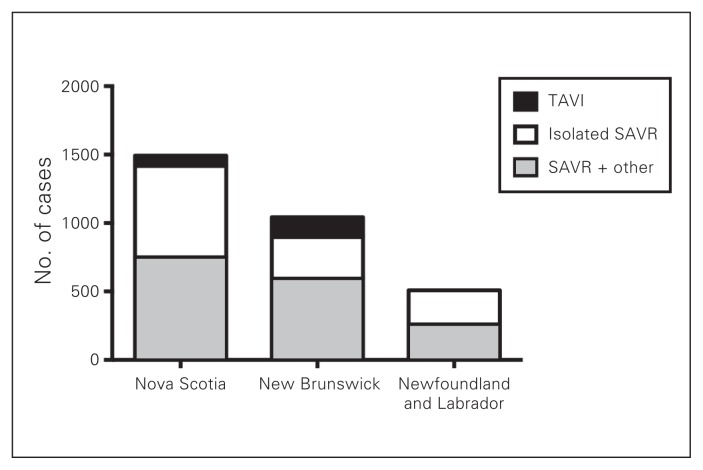
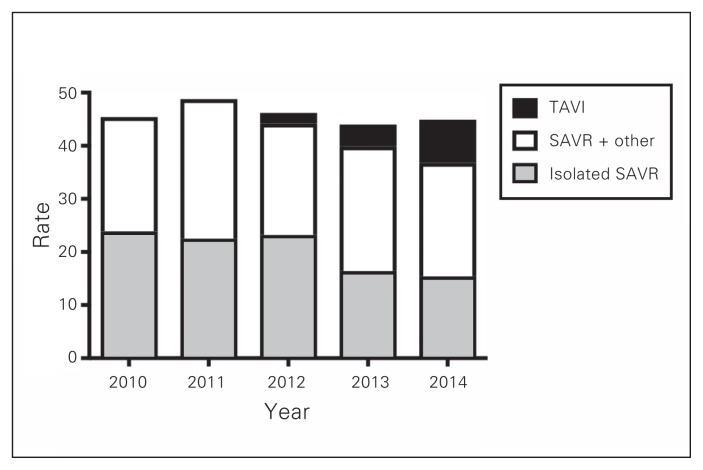
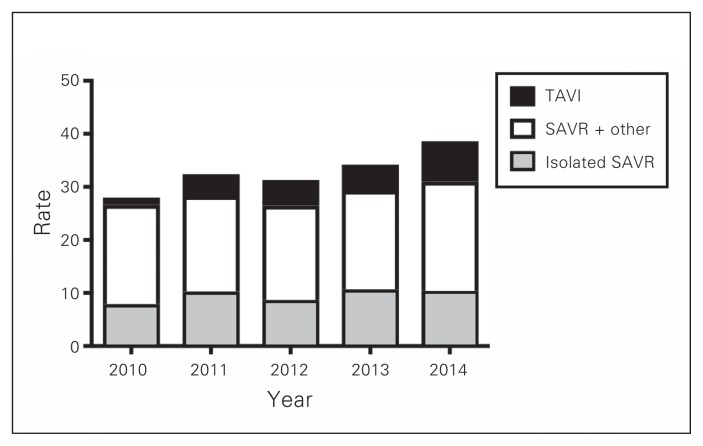
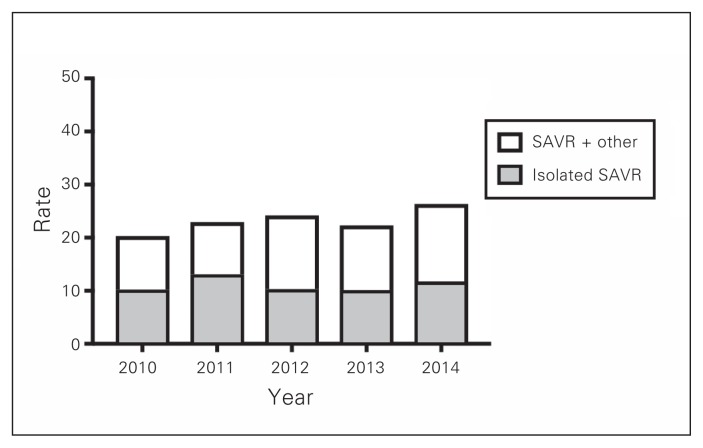
Results: A total of 3042 patients underwent SAVR or TAVI during the study period, 1491 in Nova Scotia, 1042 in New Brunswick and 509 in Newfoundland and Labrador. Patient demographic characteristics were similar across regions. A much higher proportion of patients in Newfoundland and Labrador (43.6%) than in Nova Scotia (4.2%) or New Brunswick (13.6%) received a mechanical versus a bioprosthetic valve. Rates of TAVI increased over the study period, with New Brunswick adopting their program before Nova Scotia (144 v. 74 procedures). Adjusted rates of all AVR procedures remained stable in Nova Scotia (40-50 per 100 000 people). Adjusted rates were lower in New Brunswick and Newfoundland and Labrador than in Nova Scotia; they increased slowly in New Brunswick over the study period.
Conclusion: Despite geographical proximity and similar patient demographic characteristics, there existed regional differences in the management of aortic valve disease within Atlantic Canada. Further study is required to determine whether the observed differences in age- and sex-adjusted rates of AVR may be explained by geographical disease-related differences, varying practice patterns or barriers in access to care.
Contexte: Le remplacement valvulaire aortique par cathéter, une méthode en pleine évolution, est de plus en plus utilisé pour le traitement des valvulopathies aortiques. Cette étude visait à examiner les différences régionales quant au remplacement valvulaire aortique par cathéter ou par chirurgie dans les provinces de l'Atlantique.
Méthodes: Nous avons recensé tous les patients ayant subi un remplacement valvulaire aortique entre le 1er janvier 2010 et le 31 décembre 2014 au Nouveau-Brunswick, en Nouvelle-Écosse et à Terre-Neuve-et-Labrador. Nous avons recueilli des données sur les caractéristiques démographiques des patients et les interventions chirurgicales, puis nous avons réalisé une analyse descriptive univariée et avons calculé les taux d'incidence bruts et corrigés selon l'âge et le sexe.
Résultats: En tout, 3042 patients ont subi un remplacement valvulaire aortique par cathéter ou par chirurgie pendant la période à l'étude : 1491 en Nouvelle-Écosse, 1042 au Nouveau-Brunswick et 509 à Terre-Neuve-et-Labrador. Les caractéristiques démographiques des patients étaient semblables d'une région à l'autre. La proportion des patients recevant une prothèse mécanique plutôt qu'une bioprothèse était beaucoup plus élevée à Terre-Neuve-et-Labrador (43,6 %) qu'en Nouvelle-Écosse (4,2 %) ou au Nouveau-Brunswick (13,6 %). Les taux de remplacement par cathéter ont augmenté au cours de la période à l'étude; le Nouveau-Brunswick a adopté un programme à ce sujet avant la Nouvelle-Écosse (144 c. 74 interventions). Les taux corrigés pour tous les remplacements étaient stables en Nouvelle-Écosse (40-50 par 100 000 habitants); ils étaient plus faibles au Nouveau-Brunswick et à Terre-Neuve-et-Labrador, mais ont augmenté lentement au Nouveau-Brunswick pendant la période à l'étude.
Conclusion: Malgré la proximité géographique des provinces de l'Atlantique et les caractéristiques démographiques semblables des patients, il existait des différences dans la prise en charge des valvulopathies aortiques. D'autres études seront nécessaires pour déterminer si les variations dans les taux de remplacement corrigés selon l'âge et le sexe pourraient s'expliquer par des différences géographiques dans le nombre de cas, des différences dans les pratiques ou des obstacles à l'accès aux soins.
Conflict of interest statement
Figures
References
-
- Lung B, Vahanian A. Epidemiology of acquired valvular heart disease. Can J Cardiol. 2014;30:962–70. - PubMed
-
- Quality-based procedures clinical handbook for aortic valve disease. Cardiac Care Network of Ontario & Ministry of Health and Long-Term Care; 2016. [accessed 2018 Feb 27]. Available: www.health.gov.on.ca/en/pro/programs/ecfa/docs/hb_aortic_valve_disease.pdf.
-
- Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187–98. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials