

Management of portal annular pancreas during laparoscopic pancreaticoduodenectomy
- PMID: 29582803
- PMCID: PMC6130175
- DOI: 10.4103/jmas.JMAS_235_17
Management of portal annular pancreas during laparoscopic pancreaticoduodenectomy
Abstract
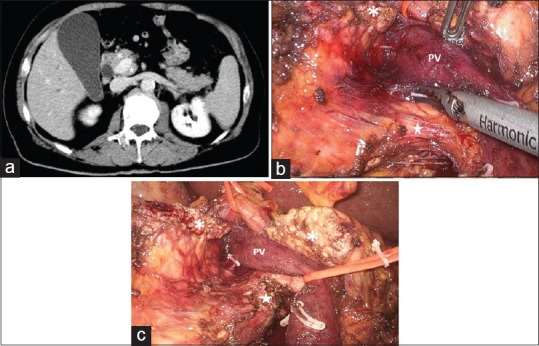
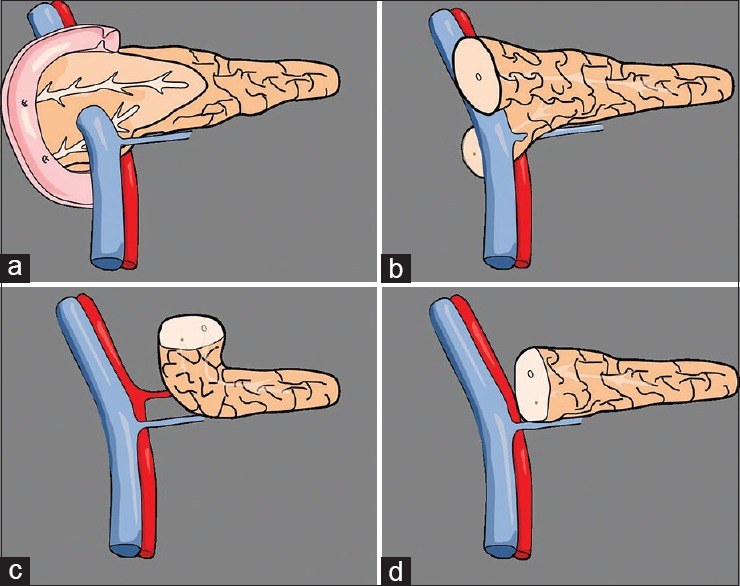
Portal annular pancreas (PAP) is a pancreatic congenital anomaly consisting of pancreatic parenchyma encircling the portal vein and/or the superior mesenteric vein. It has been reported that the risk of developing a post-operative pancreatic fistula is higher following pancreaticoduodenectomy in patients with PAP, probably because of the possibility of leaving undrained a portion of pancreatic parenchyma during the reconstructive phase. Few manuscripts have reported a surgical technique of pancreaticoduodenectomy in case of PAP, herein we report the first case of a patient with PAP undergoing laparoscopic pancreaticoduodenectomy.
Keywords: Circumportal pancreas; laparoscopic pancreaticoduodenectomy; pancreas anomaly; portal annular pancreas.
Conflict of interest statement
There are no conflicts of interest
Figures
References
-
- Karasaki H, Mizukami Y, Ishizaki A, Goto J, Yoshikawa D, Kino S, et al. Portal annular pancreas, a notable pancreatic malformation: Frequency, morphology, and implications for pancreatic surgery. Surgery. 2009;146:515–8. - PubMed
-
- Zimmitti G, Manzoni A, Addeo P, Garatti M, Zaniboni A, Bachellier P, et al. Laparoscopic pancreatoduodenectomy with superior mesenteric artery- first approach and pancreatogastrostomy assisted by mini-laparotomy. Surg Endosc. 2016;30:1670–1. - PubMed
-
- Joseph P, Raju RS, Vyas FL, Eapen A, Sitaram V. Portal annular pancreas. A rare variant and a new classification. JOP. 2010;11:453–5. - PubMed
-
- Matsumoto I, Shinzeki M, Fukumoto T, Ku Y. An extremely rare portal annular pancreas for pancreaticoduodenectomy with a special note on the pancreatic duct management in the dorsal pancreas. Surgery. 2013;153:434–6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials