

Comorbidity health pathways in heart failure patients: A sequences-of-regressions analysis using cross-sectional data from 10,575 patients in the Swedish Heart Failure Registry
- PMID: 29584734
- PMCID: PMC5870940
- DOI: 10.1371/journal.pmed.1002540
Comorbidity health pathways in heart failure patients: A sequences-of-regressions analysis using cross-sectional data from 10,575 patients in the Swedish Heart Failure Registry
Abstract
Background: Optimally treated heart failure (HF) patients often have persisting symptoms and poor health-related quality of life. Comorbidities are common, but little is known about their impact on these factors, and guideline-driven HF care remains focused on cardiovascular status. The following hypotheses were tested: (i) comorbidities are associated with more severe symptoms and functional limitations and subsequently worse patient-rated health in HF, and (ii) these patterns of association differ among selected comorbidities.
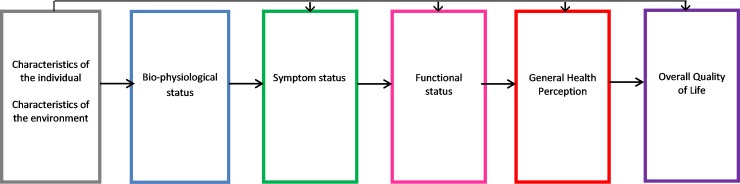
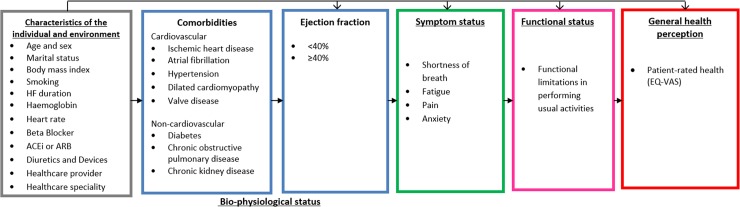
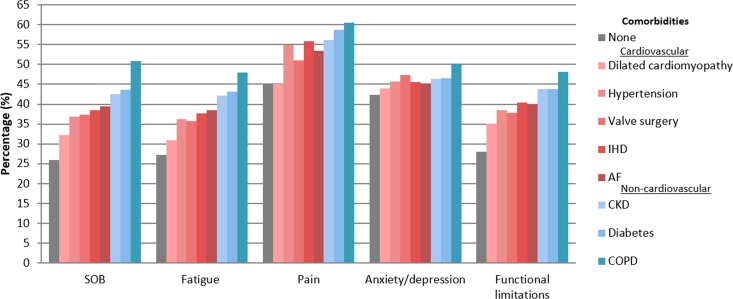
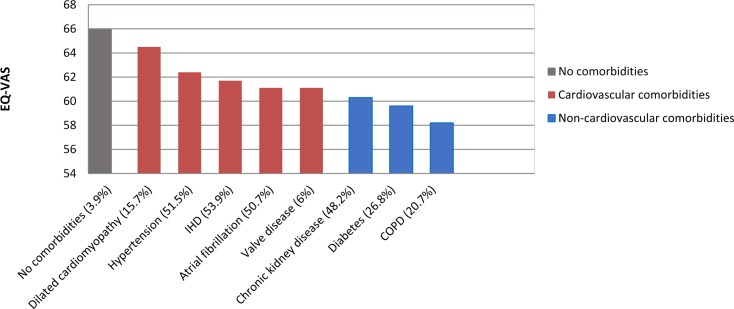
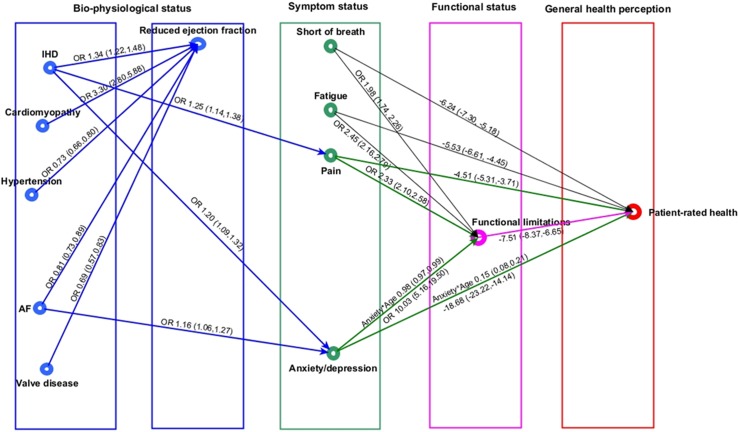
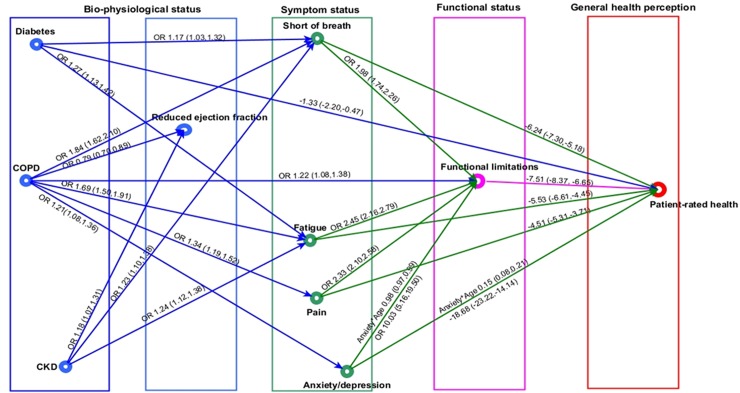
Methods and findings: The Swedish Heart Failure Registry (SHFR) is a national population-based register of HF patients admitted to >85% of hospitals in Sweden or attending outpatient clinics. This study included 10,575 HF patients with patient-rated health recorded during first registration in the SHFR (1 February 2008 to 1 November 2013). An a priori health model and sequences-of-regressions analysis were used to test associations among comorbidities and patient-reported symptoms, functional limitations, and patient-rated health. Patient-rated health measures included the EuroQol-5 dimension (EQ-5D) questionnaire and the EuroQol visual analogue scale (EQ-VAS). EQ-VAS score ranges from 0 (worst health) to 100 (best health). Patient-rated health declined progressively from patients with no comorbidities (mean EQ-VAS score, 66) to patients with cardiovascular comorbidities (mean EQ-VAS score, 62) to patients with non-cardiovascular comorbidities (mean EQ-VAS score, 59). The relationships among cardiovascular comorbidities and patient-rated health were explained by their associations with anxiety or depression (atrial fibrillation, odds ratio [OR] 1.16, 95% CI 1.06 to 1.27; ischemic heart disease [IHD], OR 1.20, 95% CI 1.09 to 1.32) and with pain (IHD, OR 1.25, 95% CI 1.14 to 1.38). Associations of non-cardiovascular comorbidities with patient-rated health were explained by their associations with shortness of breath (diabetes, OR 1.17, 95% CI 1.03 to 1.32; chronic kidney disease [CKD, OR 1.23, 95% CI 1.10 to 1.38; chronic obstructive pulmonary disease [COPD], OR 95% CI 1.84, 1.62 to 2.10) and with fatigue (diabetes, OR 1.27, 95% CI 1.13 to 1.42; CKD, OR 1.24, 95% CI 1.12 to 1.38; COPD, OR 1.69, 95% CI 1.50 to 1.91). There were direct associations between all symptoms and patient-rated health, and indirect associations via functional limitations. Anxiety or depression had the strongest association with functional limitations (OR 10.03, 95% CI 5.16 to 19.50) and patient-rated health (mean difference in EQ-VAS score, -18.68, 95% CI -23.22 to -14.14). HF optimizing therapies did not influence these associations. Key limitations of the study include the cross-sectional design and unclear generalisability to other populations. Further prospective HF studies are required to test the consistency of the relationships and their implications for health.
Conclusions: Identification of distinct comorbidity health pathways in HF could provide the evidence for individualised person-centred care that targets specific comorbidities and associated symptoms.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: Ulf Dahlstrom has no disclosures related to the present work but outside the work, he has received research grants to his institution from Astra-Zeneca, served on the speakers' bureau and received consulting fees from Astra Zeneca and Novartis.
Figures
Similar articles
-
Comorbidity and health-related quality of life in patients with severe chronic obstructive pulmonary disease attending Swedish secondary care units.Int J Chron Obstruct Pulmon Dis. 2015 Jan 22;10:173-83. doi: 10.2147/COPD.S74645. eCollection 2015. Int J Chron Obstruct Pulmon Dis. 2015. PMID: 25653516 Free PMC article.
-
Comorbid Conditions and Health-Related Quality of Life in Ambulatory Heart Failure Patients: REVIVAL (Registry Evaluation of Vital Information for VADs in Ambulatory Life REVIVAL).Circ Heart Fail. 2020 May;13(5):e006858. doi: 10.1161/CIRCHEARTFAILURE.119.006858. Epub 2020 May 18. Circ Heart Fail. 2020. PMID: 32418478 Free PMC article.
-
Health-related quality of life across heart failure categories: associations with clinical characteristics and outcomes.ESC Heart Fail. 2025 Jun;12(3):1977-1991. doi: 10.1002/ehf2.15206. Epub 2025 Jan 27. ESC Heart Fail. 2025. PMID: 39871494 Free PMC article.
-
Tailored or adapted interventions for adults with chronic obstructive pulmonary disease and at least one other long-term condition: a mixed methods review.Cochrane Database Syst Rev. 2021 Jul 26;7(7):CD013384. doi: 10.1002/14651858.CD013384.pub2. Cochrane Database Syst Rev. 2021. PMID: 34309831 Free PMC article.
-
Impact of non-cardiovascular comorbidities on the quality of life of patients with chronic heart failure: a scoping review.Health Qual Life Outcomes. 2020 Oct 7;18(1):329. doi: 10.1186/s12955-020-01566-y. Health Qual Life Outcomes. 2020. PMID: 33028351 Free PMC article.
Cited by
-
Psychosocial Syndemics and Multimorbidity in Patients with Heart Failure †.J Psychiatr Brain Sci. 2021;6:e210006. doi: 10.20900/jpbs.20210006. Epub 2021 Apr 13. J Psychiatr Brain Sci. 2021. PMID: 33954261 Free PMC article.
-
The Heart Failure "Pandemic" in Japan: Reconstruction of Health Care System in the Highly Aged Society.JMA J. 2019 Sep 4;2(2):103-112. doi: 10.31662/jmaj.2018-0049. Epub 2019 May 16. JMA J. 2019. PMID: 33615020 Free PMC article.
-
Can psychological interventions affect cardiac rehabilitation patients' well-being? Preliminary results from a longitudinal study.Int J Cardiol Cardiovasc Risk Prev. 2025 Jul 19;26:200474. doi: 10.1016/j.ijcrp.2025.200474. eCollection 2025 Sep. Int J Cardiol Cardiovasc Risk Prev. 2025. PMID: 40740290 Free PMC article.
-
Self-care behaviour and associated factors among heart failure patients in Ethiopia: a systematic review and meta-analysis.BMJ Open. 2023 Dec 10;13(12):e071960. doi: 10.1136/bmjopen-2023-071960. BMJ Open. 2023. PMID: 38072478 Free PMC article.
-
Association between β-blocker dose and quality of life after myocardial infarction: a real-world Swedish register-linked study.Eur Heart J Acute Cardiovasc Care. 2022 Jun 22;11(6):491-500. doi: 10.1093/ehjacc/zuac050. Eur Heart J Acute Cardiovasc Care. 2022. PMID: 35510962 Free PMC article.
References
-
- Alpert CM, Smith MA, Hummel SL, Hummel EK. Symptom burden in heart failure: assessment, impact on outcomes, and management. Heart Fail Rev. 2017;22(1):25–39. doi: 10.1007/s10741-016-9581-4 - DOI - PMC - PubMed
-
- Comin-Colet J, Anguita M, Formiga F, Almenar L, Crespo-Leiro MG, Manzano L, et al. Health-related quality of life of patients with chronic systolic heart failure in Spain: results of the VIDA-IC study. Rev Esp Cardiol (Engl Ed). 2016;69(3):256–71. - PubMed
-
- Lupon J, Gastelurrutia P, De Antonio M, Gonzalez B, Cano L, Cabanes R, et al. Quality of life monitoring in ambulatory heart failure patients: Temporal changes and prognostic value. Eur J Heart Fail. 2013;15(1):103–9. doi: 10.1093/eurjhf/hfs133 - DOI - PubMed
-
- Iqbal J, Francis L, Reid J, Murray S, Denvir M. Quality of life in patients with chronic heart failure and their carers: a 3-year follow-up study assessing hospitalization and mortality. Eur J Heart Fail. 2010;12(9):1002–8. doi: 10.1093/eurjhf/hfq114 - DOI - PubMed
-
- Joyce E, Chung C, Badloe S, Odutayo K, Desai A, Givertz MM, et al. Variable contribution of heart failure to quality of life in ambulatory heart failure with reduced, better, or preserved ejection fraction. JACC Heart Fail. 2016;4(3):184–93. doi: 10.1016/j.jchf.2015.12.011 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
