

Biopsy-proven vancomycin-induced acute kidney injury: a case report and literature review
- PMID: 29587650
- PMCID: PMC5872390
- DOI: 10.1186/s12882-018-0845-1
Biopsy-proven vancomycin-induced acute kidney injury: a case report and literature review
Abstract
Background: Vancomycin is the first-line antibiotic for methicillin-resistant Staphylococcus aureus and coagulase-negative strains. The risk of vancomycin-induced acute kidney injury increases with plasma vancomycin levels. Vancomycin-induced acute kidney injury is histologically characterized by acute interstitial nephritis and/or acute tubular necrosis. However, only 12 biopsy-proven cases of vancomycin-induced acute kidney injury have been reported so far, as renal biopsy is rarely performed for such cases. Current recommendations for the prevention or treatment of vancomycin-induced acute kidney injury are drug monitoring of plasma vancomycin levels using trough level and drug withdrawal. Oral prednisone and high-flux haemodialysis have led to the successful recovery of renal function in some biopsy-proven cases.
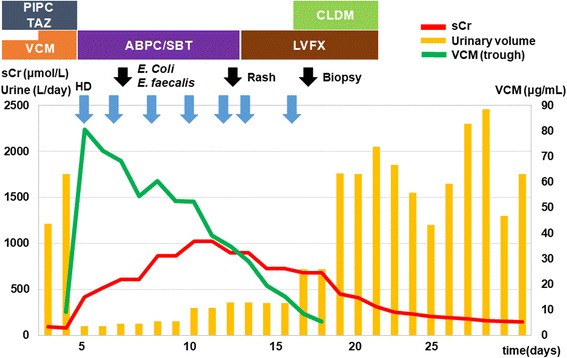
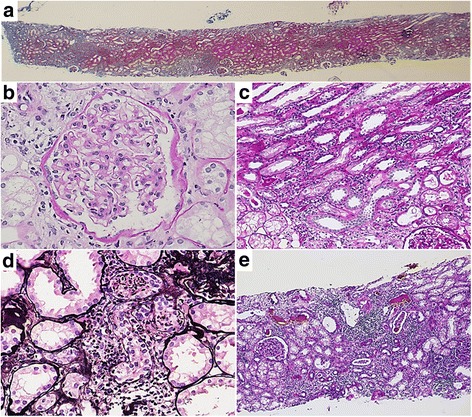
Case presentation: We present the case of a 41-year-old man with type 1 diabetes mellitus, who developed vancomycin-induced acute kidney injury during treatment for Fournier gangrene. His serum creatinine level increased to 1020.1 μmol/L from a baseline of 79.6 μmol/L, and his plasma trough level of vancomycin peaked at 80.48 μg/mL. Vancomycin discontinuation and frequent haemodialysis with high-flux membrane were immediately performed following diagnosis. Renal biopsy showed acute tubular necrosis and focal acute interstitial nephritis, mainly in the medullary rays (medullary ray injury). There was no sign of glomerulonephritis, but mild diabetic changes were detected. He was discharged without continuing haemodialysis (serum creatinine level, 145.0 μmol/L) 49 days after initial vancomycin administration.
Conclusions: This case suggests that frequent haemodialysis and renal biopsy could be useful for the treatment and assessment of vancomycin-induced acute kidney injury, particularly in high-risk cases or patients with other renal disorders.
Keywords: Acute interstitial nephritis; Acute kidney injury; Acute tubular necrosis; High-flux haemodialysis; Vancomycin.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
