

Spatiotemporal Multi-Omics Mapping Generates a Molecular Atlas of the Aortic Valve and Reveals Networks Driving Disease
- PMID: 29588317
- PMCID: PMC6160370
- DOI: 10.1161/CIRCULATIONAHA.117.032291
Spatiotemporal Multi-Omics Mapping Generates a Molecular Atlas of the Aortic Valve and Reveals Networks Driving Disease
Abstract
Background: No pharmacological therapy exists for calcific aortic valve disease (CAVD), which confers a dismal prognosis without invasive valve replacement. The search for therapeutics and early diagnostics is challenging because CAVD presents in multiple pathological stages. Moreover, it occurs in the context of a complex, multi-layered tissue architecture; a rich and abundant extracellular matrix phenotype; and a unique, highly plastic, and multipotent resident cell population.
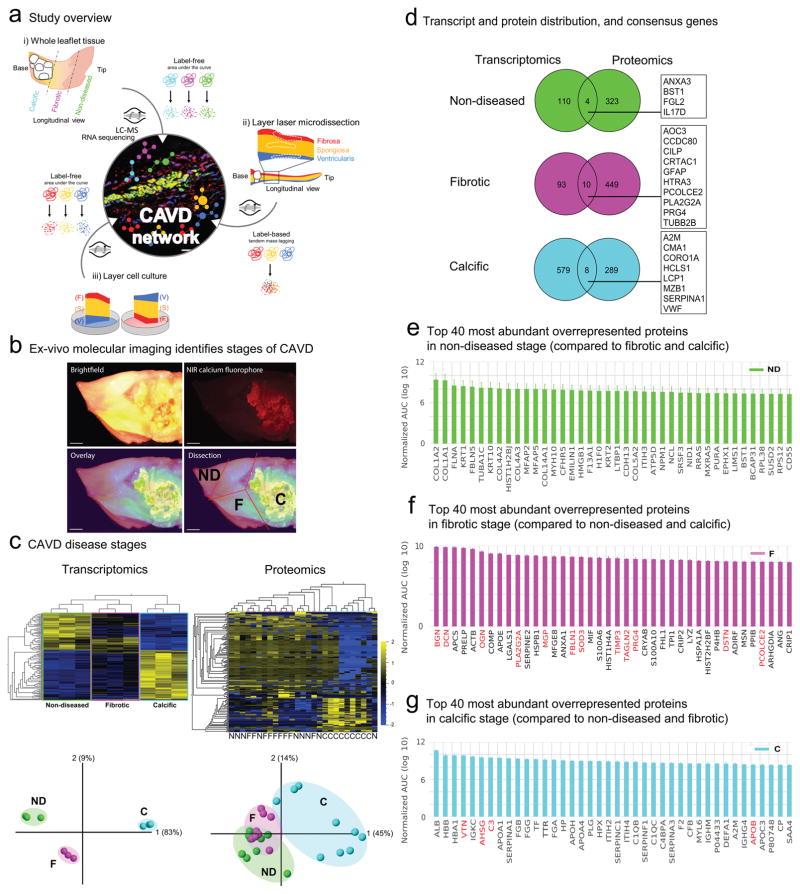
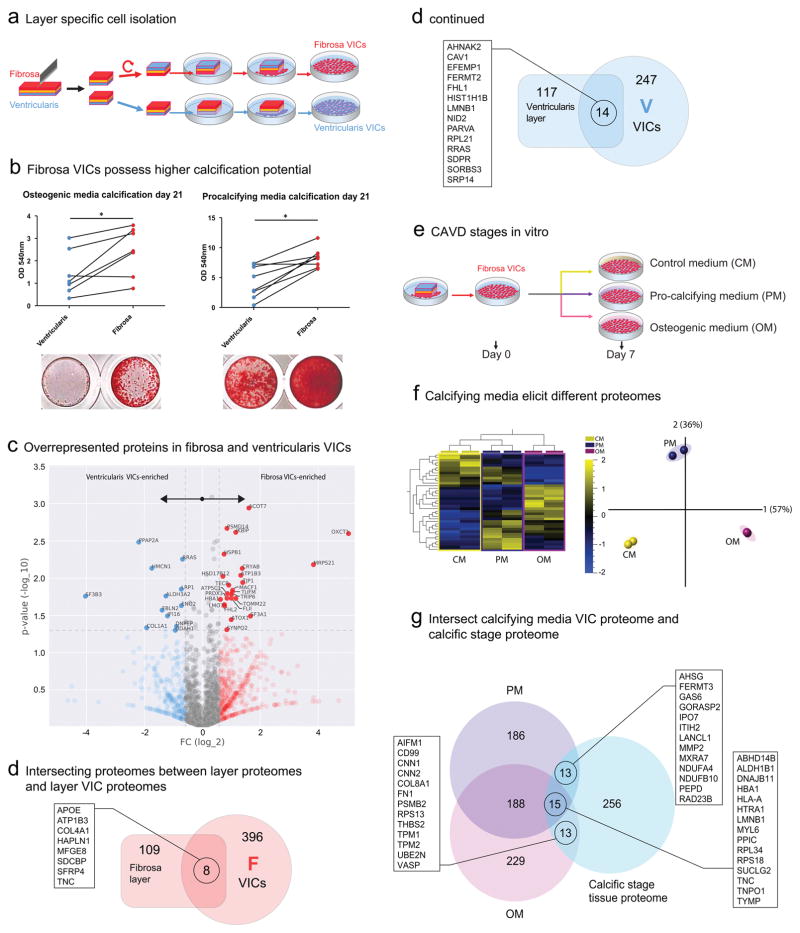
Methods: A total of 25 human stenotic aortic valves obtained from valve replacement surgeries were analyzed by multiple modalities, including transcriptomics and global unlabeled and label-based tandem-mass-tagged proteomics. Segmentation of valves into disease stage-specific samples was guided by near-infrared molecular imaging, and anatomic layer-specificity was facilitated by laser capture microdissection. Side-specific cell cultures were subjected to multiple calcifying stimuli, and their calcification potential and basal/stimulated proteomes were evaluated. Molecular (protein-protein) interaction networks were built, and their central proteins and disease associations were identified.
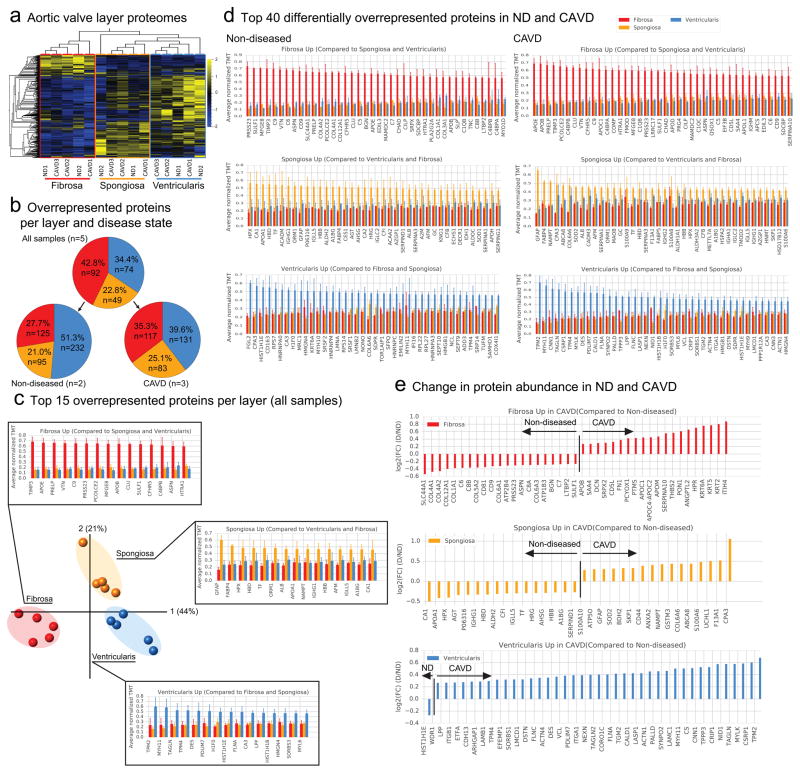
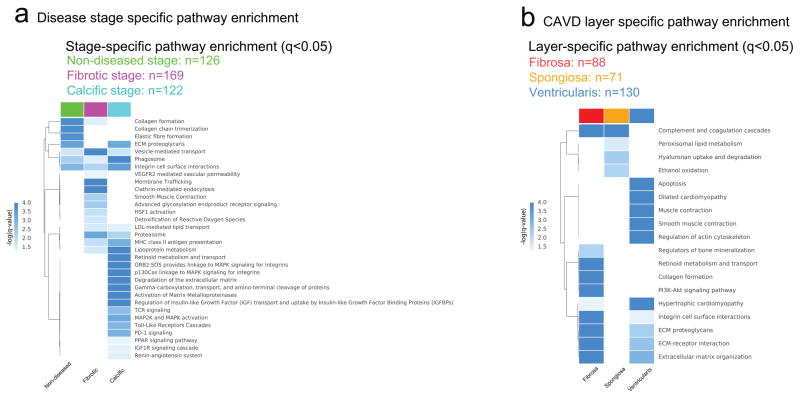
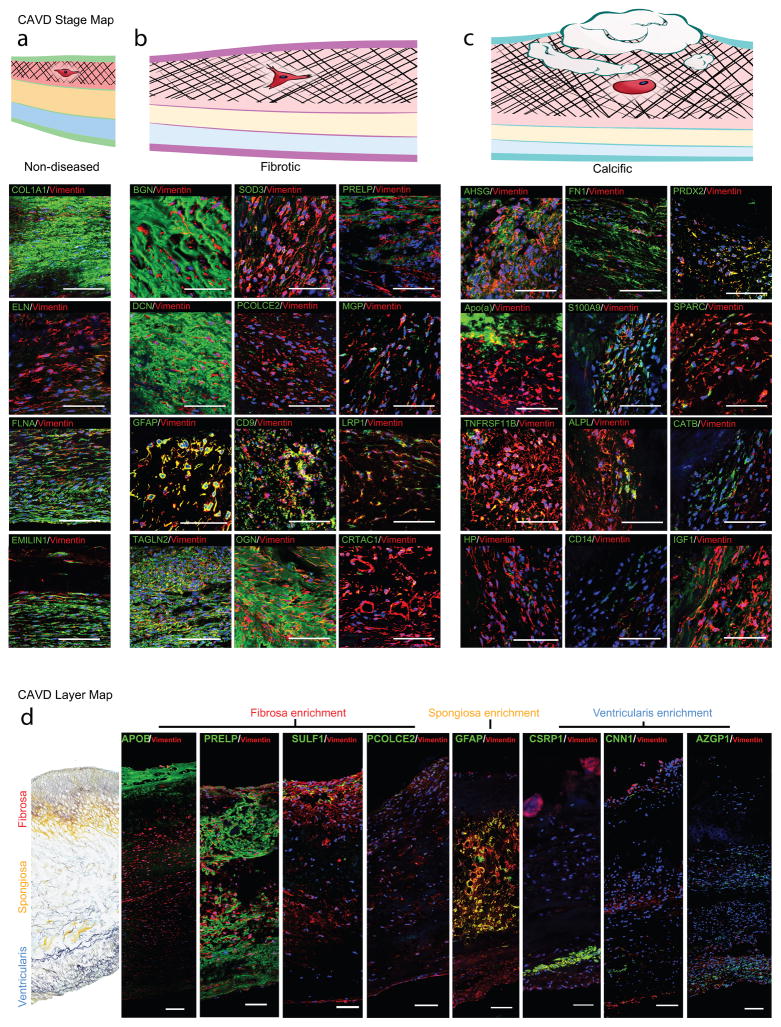
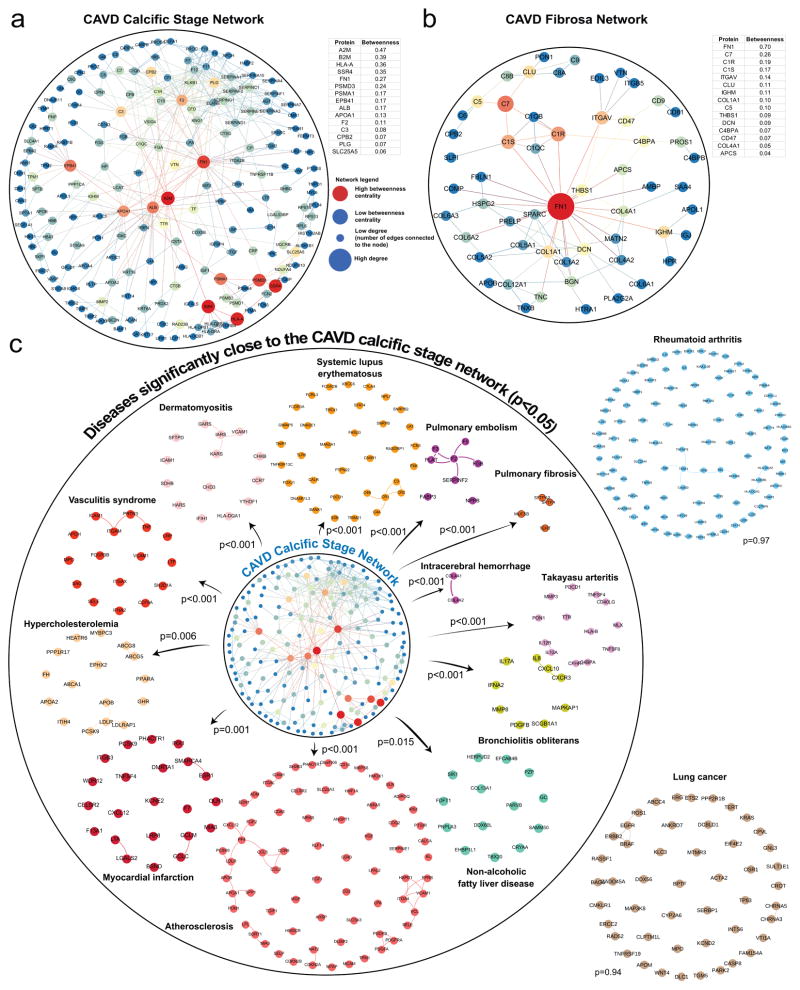
Results: Global transcriptional and protein expression signatures differed between the nondiseased, fibrotic, and calcific stages of CAVD. Anatomic aortic valve microlayers exhibited unique proteome profiles that were maintained throughout disease progression and identified glial fibrillary acidic protein as a specific marker of valvular interstitial cells from the spongiosa layer. CAVD disease progression was marked by an emergence of smooth muscle cell activation, inflammation, and calcification-related pathways. Proteins overrepresented in the disease-prone fibrosa are functionally annotated to fibrosis and calcification pathways, and we found that in vitro, fibrosa-derived valvular interstitial cells demonstrated greater calcification potential than those from the ventricularis. These studies confirmed that the microlayer-specific proteome was preserved in cultured valvular interstitial cells, and that valvular interstitial cells exposed to alkaline phosphatase-dependent and alkaline phosphatase-independent calcifying stimuli had distinct proteome profiles, both of which overlapped with that of the whole tissue. Analysis of protein-protein interaction networks found a significant closeness to multiple inflammatory and fibrotic diseases.
Conclusions: A spatially and temporally resolved multi-omics, and network and systems biology strategy identifies the first molecular regulatory networks in CAVD, a cardiac condition without a pharmacological cure, and describes a novel means of systematic disease ontology that is broadly applicable to comprehensive omics studies of cardiovascular diseases.
Keywords: aortic valve; network medicine; proteomics; stenosis; transcriptomics; vascular calcification.
Figures
Comment in
-
Spatiotemporal Multi-Omics-Derived Atlas of Calcific Aortic Valve Disease.Circulation. 2018 Jul 24;138(4):394-396. doi: 10.1161/CIRCULATIONAHA.118.035431. Circulation. 2018. PMID: 30571374 Free PMC article. No abstract available.
References
-
- Stewart BF, Siscovick D, Lind BK, Gardin JM, Gottdiener JS, Smith VE, Kitzman DW, Otto CM. Clinical factors associated with calcific aortic valve disease. J Am Coll Cardiol. 1997;29:630–634. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, 3rd, Guyton RA, O’Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM, 3rd, Thomas JD. 2014 aha/acc guideline for the management of patients with valvular heart disease: Executive summary: A report of the american college of cardiology/american heart association task force on practice guidelines. Circulation. 2014;129:2440–2492. - PubMed
-
- Ross J, Braunwald E. Aortic stenosis. Circulation. 1968;38:V-61–V-67. - PubMed
-
- Schoen FJ. Evolving concepts of cardiac valve dynamics. Circulation. 2008;118:1864. - PubMed
-
- Otto CM, Kuusisto J, Reichenbach DD, Gown AM, O’Brien KD. Characterization of the early lesion of ‘degenerative’ valvular aortic stenosis. Histological and immunohistochemical studies. Circulation. 1994;90:844–853. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
