

Standing Practice In Rehabilitation Early after Stroke (SPIRES): a functional standing frame programme (prolonged standing and repeated sit to stand) to improve function and quality of life and reduce neuromuscular impairment in people with severe sub-acute stroke-a protocol for a feasibility randomised controlled trial
- PMID: 29588861
- PMCID: PMC5865293
- DOI: 10.1186/s40814-018-0254-z
Standing Practice In Rehabilitation Early after Stroke (SPIRES): a functional standing frame programme (prolonged standing and repeated sit to stand) to improve function and quality of life and reduce neuromuscular impairment in people with severe sub-acute stroke-a protocol for a feasibility randomised controlled trial
Abstract
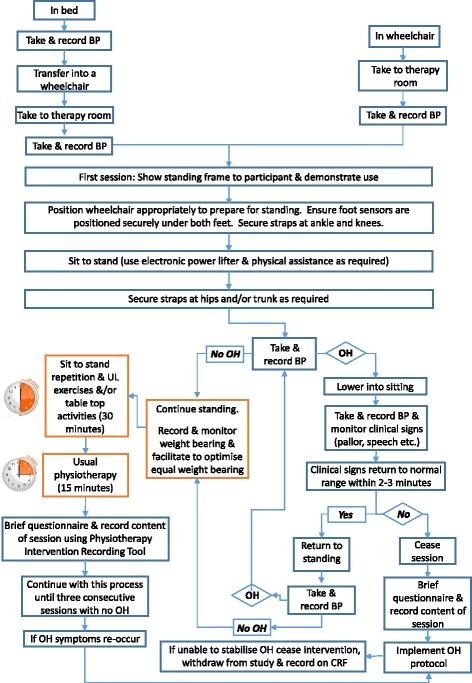
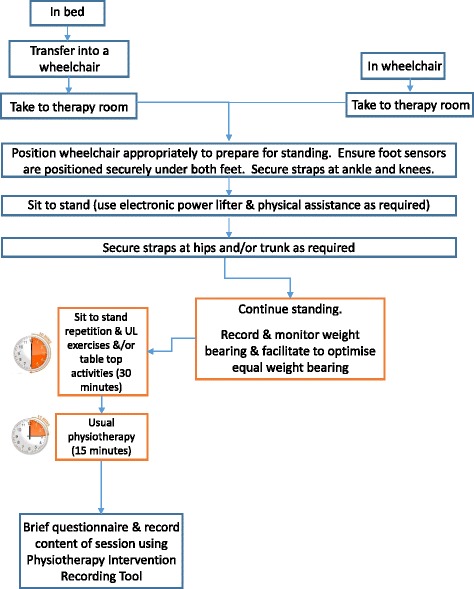
Background: The most common physical deficit caused by a stroke is muscle weakness which limits a person's mobility. Mobility encompasses activities necessary for daily functioning: getting in and out bed, on/off toilet, sitting, standing and walking. These activities are significantly affected in people with severe stroke who typically spend most of their time in bed or a chair and are immobile. Immobility is primarily caused by neurological damage but exacerbated by secondary changes in musculoskeletal and cardiorespiratory systems. These secondary changes can theoretically be prevented or minimised by early mobilisation, in this case standing up early post-stroke.Standing up early post-stroke has been identified as an important priority for people who have suffered a severe stroke. However, trials of prolonged passive standing have not demonstrated any functional improvements. Conversely, task-specific training such as repeated sit-to-stand has demonstrated positive functional benefits. This feasibility trial combines prolonged standing and task-specific strength training with the aim of determining whether this novel combination of physiotherapy interventions is feasible for people with severe stroke as well as the overall feasibility of delivering the trial.
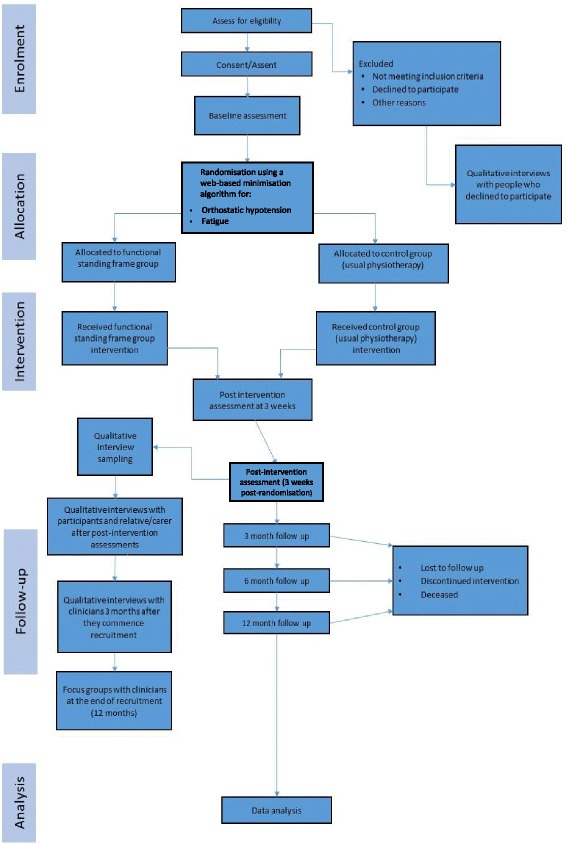
Methods/design: This is a pragmatic multi-centre parallel single-blinded two-armed feasibility randomised controlled trial. Fifty people with a diagnosis of severe stroke will be randomly allocated to either the functional standing frame programme or usual physiotherapy. All patient participants will be assessed at baseline and followed up at 3 weeks, then 3, 6 and 12 months post-randomisation. Trial objectives are to determine the feasibility according to the following indicators:: (i) Process: recruitment and retention rate, ability to consent, eligibility criteria, willingness/ability of physiotherapists to recruit, willingness of patients to be randomised, and acceptability of the intervention; (ii) Resource: burden and potential costs; (iii) Management: treatment fidelity, participant adherence, acceptability and completeness of outcome measures, impact and management or orthostatic hypotension; and (iv) Safety: number and nature of adverse and serious adverse events.
Discussion: The functional standing frame programme addresses a key concern for people who have suffered a severe stroke. However, several uncertainties exist which need to be understood prior to progressing to a full-scale trial, including acceptability and tolerance of the functional standing frame programme intervention and practicality of the trial procedures. This feasibility trial will provide important insights to resolve these uncertainties.
Trial registration: International Standard Randomised Controlled Trial Number ISRCTN15412695. Registration on 19 December 2016.
Keywords: Early mobilisation; Feasibility randomised controlled trial; Function; Neuromuscular impairment; Physiotherapy; Stroke; Supported standing.
Conflict of interest statement
The authors declare the trial protocol, participant information and enrolment procedures were assessed and approved through the National Research Ethics Scheme (NRES Committee Wales, Reference number: 16/WA/0229 and the Health Research Authority (HRA), Reference number: 201646). Any amendments to the protocol will be reported to and approved via NRES and the HRA.NIHR have approved this publication.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Baker K, Cassidy E, Rone-Adams S. Therapeutic standing for people with multiple sclerosis: efficacy and feasibility. Int J Ther Rehabil. 2013;14(3)
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
