

Multimodal, automated detection of nocturnal motor seizures at home: Is a reliable seizure detector feasible?
- PMID: 29588973
- PMCID: PMC5862103
- DOI: 10.1002/epi4.12076
Multimodal, automated detection of nocturnal motor seizures at home: Is a reliable seizure detector feasible?
Abstract
Objective: Automated seizure detection and alarming could improve quality of life and potentially prevent sudden, unexpected death in patients with severe epilepsy. As currently available systems focus on tonic-clonic seizures, we want to detect a broader range of seizure types, including tonic, hypermotor, and clusters of seizures.
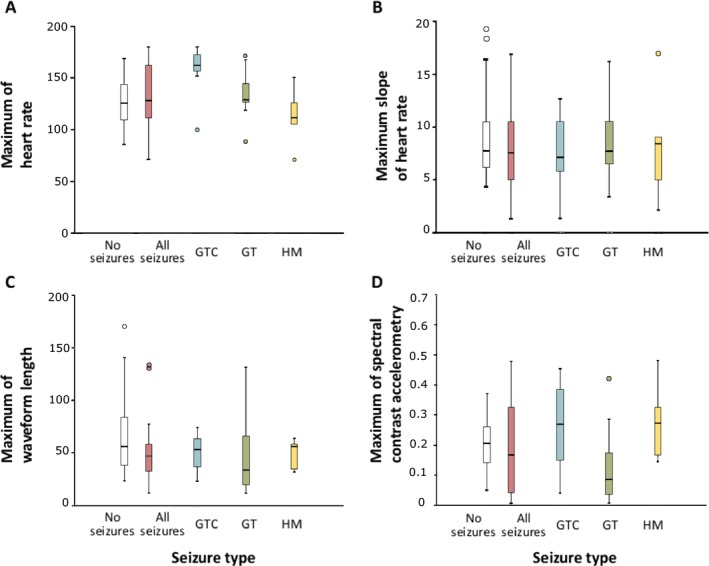
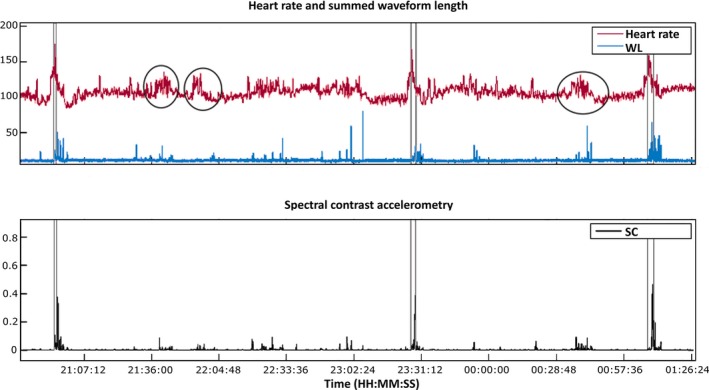
Methods: In this multicenter, prospective cohort study, the nonelectroencephalographic (non-EEG) signals heart rate and accelerometry were measured during the night in patients undergoing a diagnostic video-EEG examination. Based on clinical video-EEG data, seizures were classified and categorized as clinically urgent or not. Seizures included for analysis were tonic, tonic-clonic, hypermotor, and clusters of short myoclonic/tonic seizures. Features reflecting physiological changes in heart rate and movement were extracted. Detection algorithms were developed based on stepwise fulfillment of conditions during increases in either feature. A training set was used for development of algorithms, and an independent test set was used for assessing performance.
Results: Ninety-five patients were included, but due to sensor failures, data from only 43 (of whom 23 patients had 86 seizures, representing 402 h of data) could be used for analysis. The algorithms yield acceptable sensitivities, especially for clinically urgent seizures (sensitivity = 71-87%), but produce high false alarm rates (2.3-5.7 per night, positive predictive value = 25-43%). There was a large variation in the number of false alarms per patient.
Significance: It seems feasible to develop a detector with high sensitivity, but false alarm rates are too high for use in clinical practice. For further optimization, personalization of algorithms may be necessary.
Keywords: Accelerometry; Epilepsy; Heart rate; Seizure monitoring; Sudden unexpected death in epilepsy.
Figures
References
-
- Löscher W, Schmidt D. Modern antiepileptic drug development has failed to deliver: ways out of the current dilemma. Epilepsia 2011;52:657–678. - PubMed
-
- Lamberts RJ, Thijs RD, Laffan A, et al. Sudden unexpected death in epilepsy: people with nocturnal seizures may be at highest risk. Epilepsia 2012;53:253–257. - PubMed
-
- Ryvlin P, Nashef L, Lhatoo SD, et al. Incidence and mechanisms of cardiorespiratory arrests in epilepsy monitoring units (MORTEMUS): a retrospective study. Lancet Neurol 2013;12:966–977. - PubMed
-
- Hoppe C, Poepel A, Elger CE. Accuracy of patient seizure counts. Arch Neurol 2007;64:1595–1599. - PubMed
-
- Osorio I, Schachter S. Extracerebral detection of seizures: a new era in epileptology? Epilepsy Behav 2011;22(suppl 1):S82–S87. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
