

Maintenance fluid therapy and fluid creep impose more significant fluid, sodium, and chloride burdens than resuscitation fluids in critically ill patients: a retrospective study in a tertiary mixed ICU population
- PMID: 29589054
- PMCID: PMC5924672
- DOI: 10.1007/s00134-018-5147-3
Maintenance fluid therapy and fluid creep impose more significant fluid, sodium, and chloride burdens than resuscitation fluids in critically ill patients: a retrospective study in a tertiary mixed ICU population
Abstract
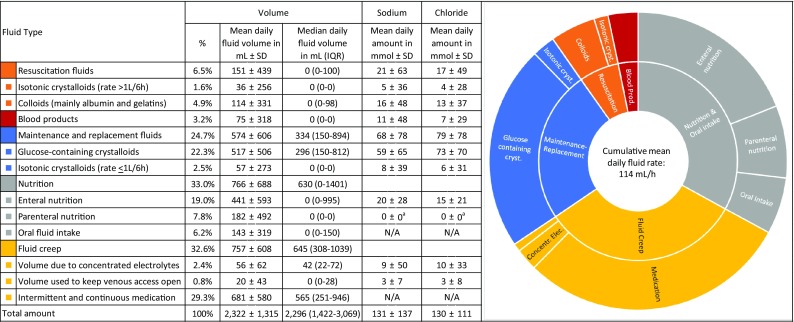
Purpose: Research on intravenous fluid therapy and its side effects, volume, sodium, and chloride overload, has focused almost exclusively on the resuscitation setting. We aimed to quantify all fluid sources in the ICU and assess fluid creep, the hidden and unintentional volume administered as a vehicle for medication or electrolytes.
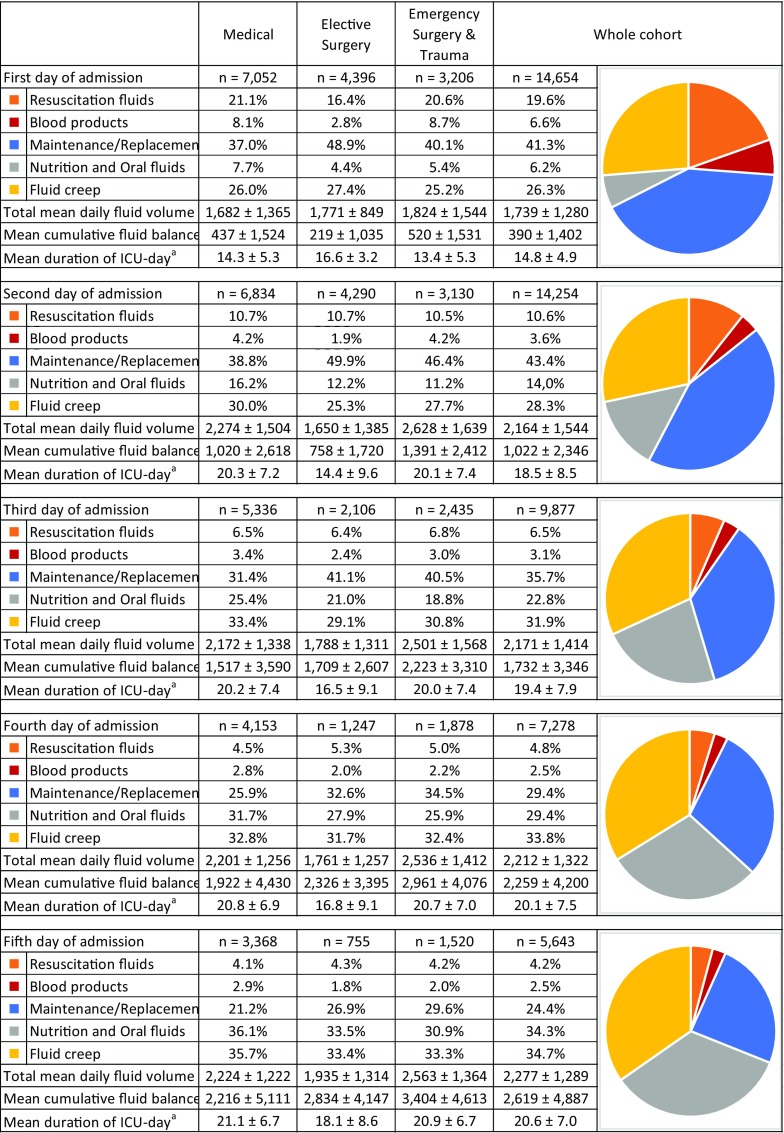
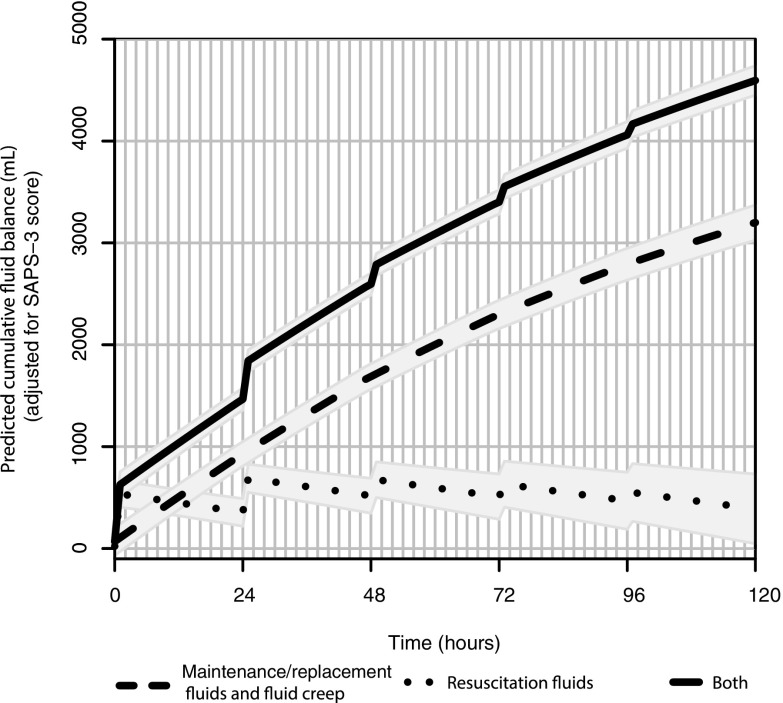
Methods: We precisely recorded the volume, sodium, and chloride burdens imposed by every fluid source administered to 14,654 patients during the cumulative 103,098 days they resided in our 45-bed tertiary ICU and simulated the impact of important strategic fluid choices on patients' chloride burdens. In septic patients, we assessed the impact of the different fluid sources on cumulative fluid balance, an established marker of morbidity.
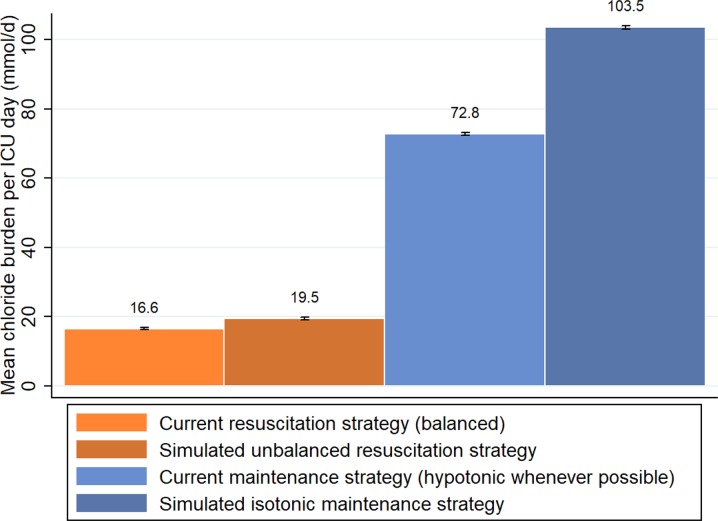
Results: Maintenance and replacement fluids accounted for 24.7% of the mean daily total fluid volume, thereby far exceeding resuscitation fluids (6.5%) and were the most important sources of sodium and chloride. Fluid creep represented a striking 32.6% of the mean daily total fluid volume [median 645 mL (IQR 308-1039 mL)]. Chloride levels can be more effectively reduced by adopting a hypotonic maintenance strategy [a daily difference in chloride burden of 30.8 mmol (95% CI 30.5-31.1)] than a balanced resuscitation strategy [daily difference 3.0 mmol (95% CI 2.9-3.1)]. In septic patients, non-resuscitation fluids had a larger absolute impact on cumulative fluid balance than did resuscitation fluids.
Conclusions: Inadvertent daily volume, sodium, and chloride loading should be avoided when prescribing maintenance fluids in view of the vast amounts of fluid creep. This is especially important when adopting an isotonic maintenance strategy.
Keywords: Chloride; Fluid creep; Fluid overload; Fluid therapy; Hyperchloremia; Maintenance fluids; Sodium.
Conflict of interest statement
All authors declare that they have no conflicts of interest.
Figures
References
-
- Young P, Bailey M, Beasley R, Henderson S, Mackle D, McArthur C, et al. Effect of a buffered crystalloid solution vs saline on acute kidney injury among patients in the intensive care unit: the SPLIT randomized clinical trial. JAMA. 2015;314(16):1701–1710. doi: 10.1001/jama.2015.12334. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
