

Benefit Versus Risk Assessment of Rotavirus Vaccination in France: A Simulation and Modeling Analysis
- PMID: 29589230
- PMCID: PMC5878204
- DOI: 10.1007/s40259-018-0273-6
Benefit Versus Risk Assessment of Rotavirus Vaccination in France: A Simulation and Modeling Analysis
Abstract
Introduction: Two vaccines against rotavirus gastroenteritis (RVGE) in young children, Rotarix and RotaTeq, have been available in Europe since 2006. Vaccination against rotaviruses significantly reduces the burden of RVGE, but it is also associated with a very small increased risk of intussusception. In a benefit-risk analysis, the prevented RVGE burden is weighed against the possible excess of intussusception.
Purpose: The aim was to compare the estimated benefits and risks of Rotarix vaccination in France.
Methods: We estimated the benefits (vaccine-preventable RVGE hospitalizations and deaths) and risks (vaccine-caused intussusception hospitalizations and deaths) following two doses of Rotarix in a birth cohort of 791,183 followed for 3-5 years in France. We used data from peer-reviewed clinical and epidemiological studies or publications, and government statistics.
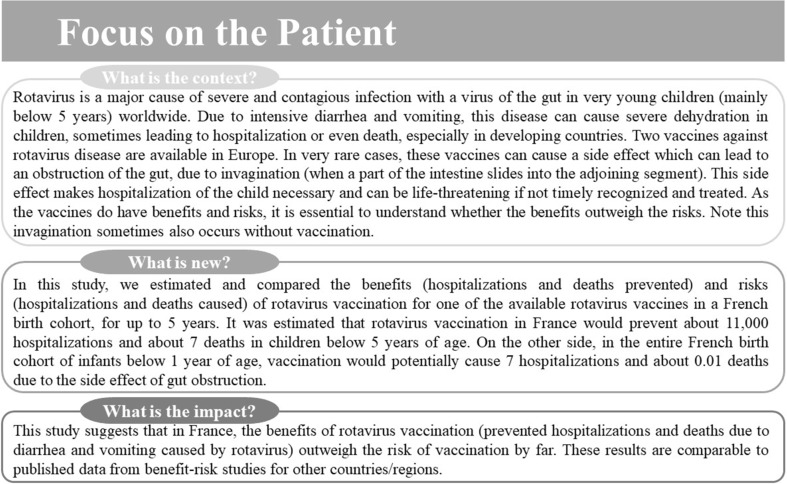
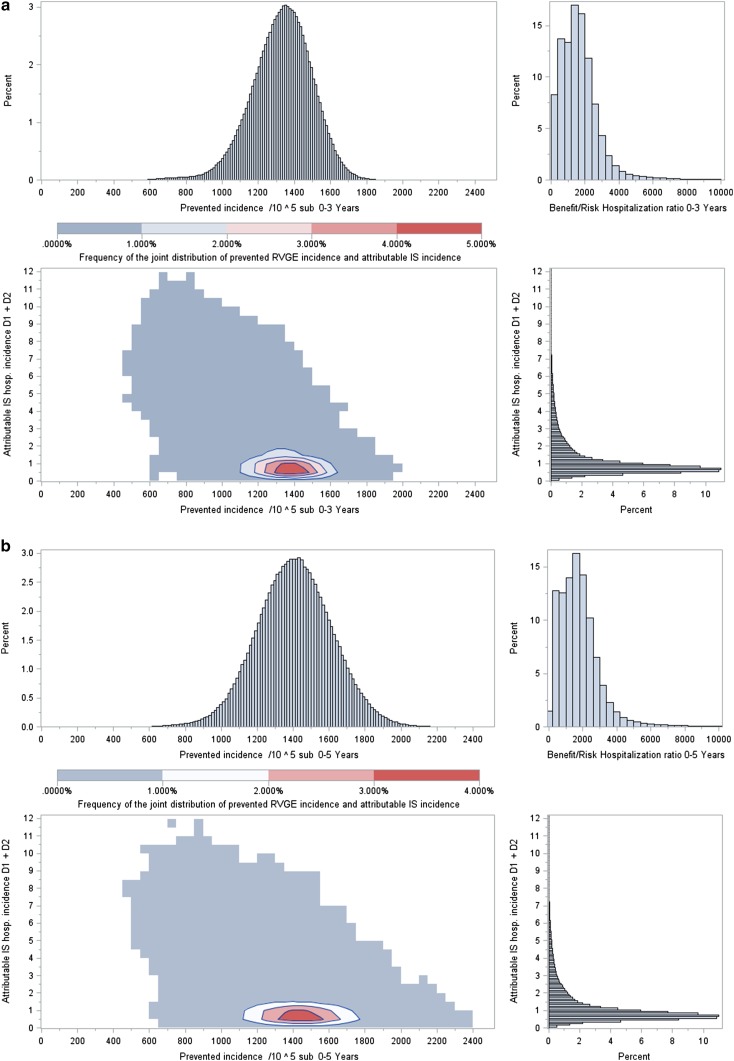
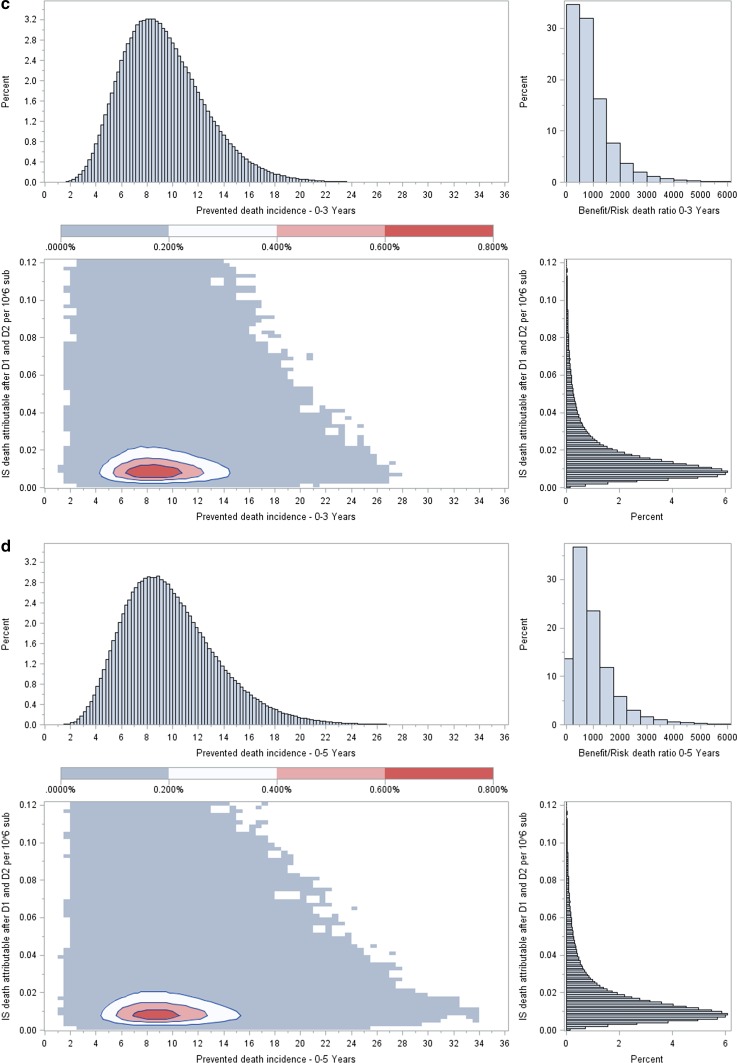
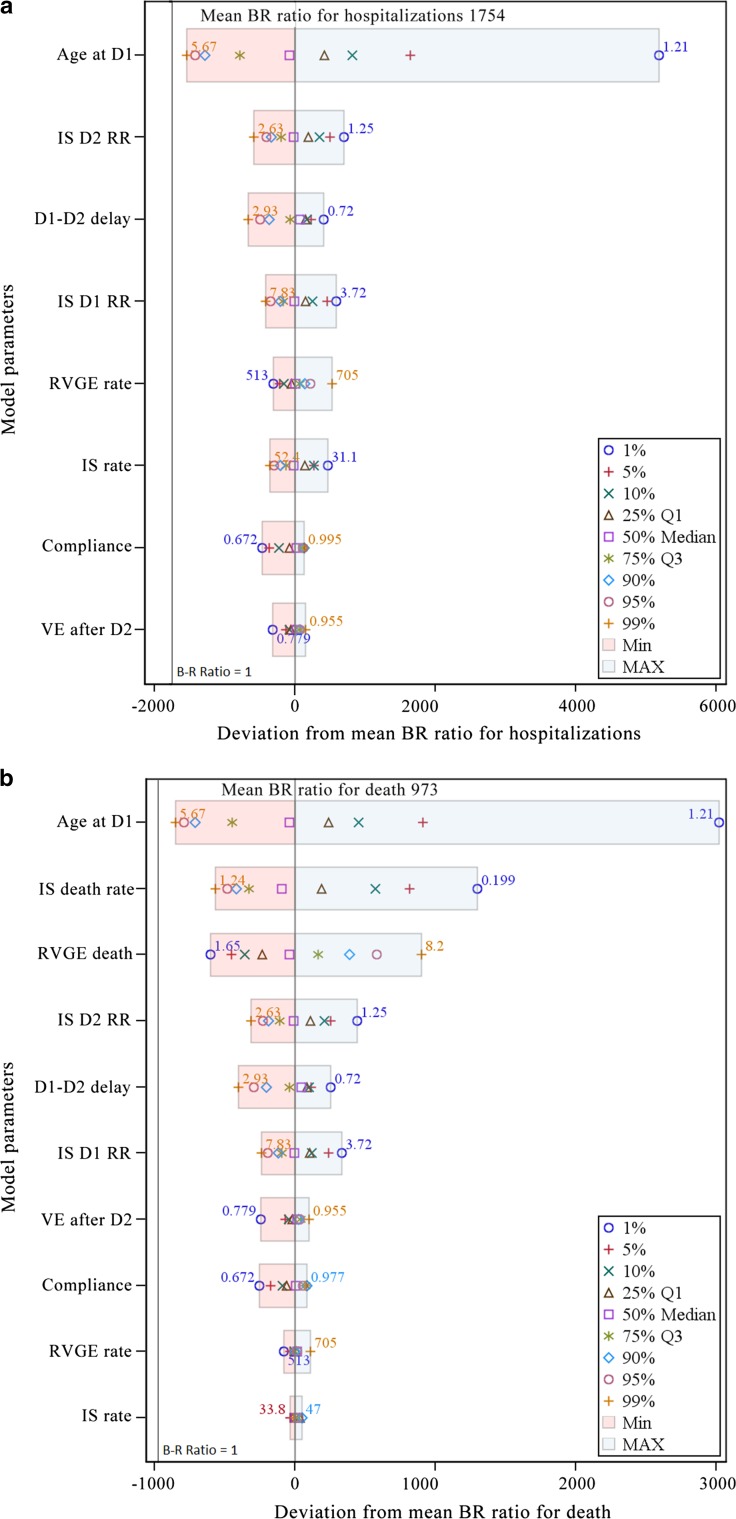
Results: Within the total number of French children below 5 years of age, we estimate vaccination could prevent a median 11,132 [95% credible interval (CI) 7842-14,408] RVGE hospitalizations and 7.43 (95% CI 3.27-14.68) RVGE deaths. At the same time, vaccination could cause an average of 6.86 (95% CI 2.25-38.37) intussusception hospitalizations and 0.0099 (95% CI 0.0024-0.060) intussusception deaths in the entire French birth cohort of infants below 1 year of age. Therefore, for every intussusception hospitalization and every intussusception death caused by vaccination, 1624 (95% CI 240-5243) RVGE hospitalizations and 743 (95% CI 93-3723) RVGE deaths are prevented, respectively, by vaccination.
Conclusions: The vaccine-prevented RVGE hospitalizations and deaths (benefit) greatly outweigh the excess potentially vaccination-related cases of intussusception (risk), indicating a favorable benefit-risk balance for Rotarix in France.
Conflict of interest statement
Conflict of interest
Edouard Ledent, Hugo Arlegui, Hubert Buyse, Naveen Karkada, Gaëlle Nachbaur and Nicolas Praet are employed by the GSK group of companies. Hubert Buyse, Edouard Ledent, Gaëlle Nachbaur and Nicolas Praet also hold shares in the GSK group of companies. Peter Basile was an employee of the GSK group of companies at the time of the study and also held shares in the GSK group of companies. Hugo Arlegui is also a doctoral fellow whose research is financed by the Association Nationale pour la Recherche et la Technologie (ANRT) (Paris, France) and the GSK group of companies.
Funding
GlaxoSmithKline Biologicals SA was the funding source and was involved in all stages of study conduct and analysis. GlaxoSmithKline Biologicals SA also funded all costs associated with the development and the publishing of the present manuscript.
Trademarks
Rotarix is a trademark of the GSK group of companies. RotaTeq is a trademark of Merck & Co., Inc.
Figures
References
-
- Sanderson C, Clark A, Taylor D, Bolanos B. Global review of rotavirus morbidity and mortality data by age and region. In: Report to WHO/IVB. 2011. http://www.who.int/immunization/sage/meetings/2012/april/Sanderson_et_al.... Accessed 10 Oct 2017.
-
- Tate JE, Burton AH, Boschi-Pinto C, Steele AD, Duque J, Parashar UD. 2008 estimate of worldwide rotavirus-associated mortality in children younger than 5 years before the introduction of universal rotavirus vaccination programmes: a systematic review and meta-analysis. Lancet Infect Dis. 2012;12(2):136–141. doi: 10.1016/S1473-3099(11)70253-5. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
