

Alveolar leak develops by a rich-get-richer process in ventilator-induced lung injury
- PMID: 29590136
- PMCID: PMC5874026
- DOI: 10.1371/journal.pone.0193934
Alveolar leak develops by a rich-get-richer process in ventilator-induced lung injury
Abstract
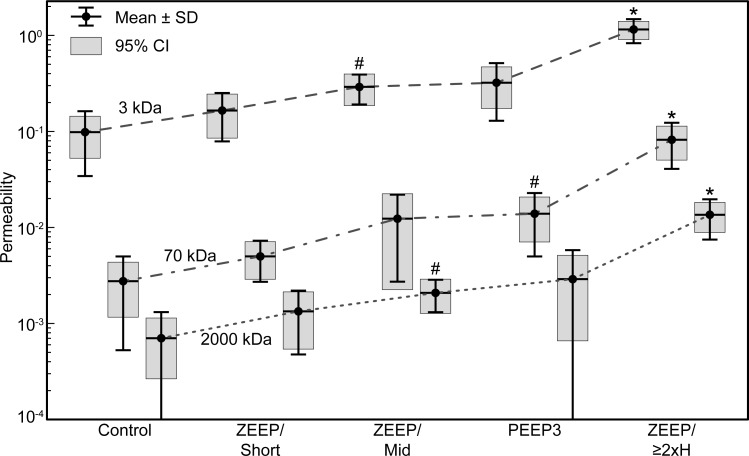
Acute respiratory distress syndrome (ARDS) is a life-threatening condition for which there are currently no medical therapies other than supportive care involving the application of mechanical ventilation. However, mechanical ventilation itself can worsen ARDS by damaging the alveolocapillary barrier in the lungs. This allows plasma-derived fluid and proteins to leak into the airspaces of the lung where they interfere with the functioning of pulmonary surfactant, which increases the stresses of mechanical ventilation and worsens lung injury. Once such ventilator-induced lung injury (VILI) is underway, managing ARDS and saving the patient becomes increasingly problematic. Maintaining an intact alveolar barrier thus represents a crucial management goal, but the biophysical processes that perforate this barrier remain incompletely understood. To study the dynamics of barrier perforation, we subjected initially normal mice to an injurious ventilation regimen that imposed both volutrauma (overdistension injury) and atelectrauma (injury from repetitive reopening of closed airspaces) on the lung, and observed the rate at which macromolecules of various sizes leaked into the airspaces as a function of the degree of overall injury. Computational modeling applied to our findings suggests that perforations in the alveolocapillary barrier appear and progress according to a rich-get-richer mechanism in which the likelihood of a perforation getting larger increases with the size of the perforation. We suggest that atelectrauma causes the perforations after which volutrauma expands them. This mechanism explains why atelectrauma appears to be essential to the initiation of VILI in a normal lung, and why atelectrauma and volutrauma then act synergistically once VILI is underway.
Conflict of interest statement
Figures

References
-
- Force ADT, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–33. doi: 10.1001/jama.2012.5669 . - DOI - PubMed
-
- Thammanomai A, Hamakawa H, Bartolak-Suki E, Suki B. Combined effects of ventilation mode and positive end-expiratory pressure on mechanics, gas exchange and the epithelium in mice with acute lung injury. PLoS One. 2013;8(1):e53934 doi: 10.1371/journal.pone.0053934 ; PubMed Central PMCID: PMCPMC3541132. - DOI - PMC - PubMed
-
- Holm BA, Enhorning G, Notter RH. A biophysical mechanism by which plasma proteins inhibit lung surfactant activity. Chem Phys Lipids. 1988;49(1–2):49–55. . - PubMed
-
- Gunther A, Siebert C, Schmidt R, Ziegler S, Grimminger F, Yabut M, et al. Surfactant alterations in severe pneumonia, acute respiratory distress syndrome, and cardiogenic lung edema. Am J Respir Crit Care Med. 1996;153(1):176–84. doi: 10.1164/ajrccm.153.1.8542113 . - DOI - PubMed
-
- Smith BJ, Bartolak-Suki E, Suki B, Roy GS, Hamlington KL, Charlebois CM, et al. Linking Ventilator Injury-Induced Leak across the Blood-Gas Barrier to Derangements in Murine Lung Function. Front Physiol. 2017;8:466 Epub 2017/07/25. doi: 10.3389/fphys.2017.00466 ; PubMed Central PMCID: PMCPMC5500660. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
