

Pre-treatment tumour perfusion parameters and initial RECIST response do not predict long-term survival outcomes for patients with head and neck squamous cell carcinoma treated with induction chemotherapy
- PMID: 29590180
- PMCID: PMC5874054
- DOI: 10.1371/journal.pone.0194841
Pre-treatment tumour perfusion parameters and initial RECIST response do not predict long-term survival outcomes for patients with head and neck squamous cell carcinoma treated with induction chemotherapy
Abstract
Objectives: Previously, we showed that pre-treatment tumour plasma perfusion (Fp) predicts RECIST response to induction chemotherapy (ICT) in locoregionally advanced head and neck squamous cell carcinoma (HNSCC). The aim here was to determine whether the pre-treatment tumour Fp estimate, changes in tumour Fp or RECIST response post 2 cycles of ICT were prognostic for long-term survival outcomes.
Methods: A prospective study enrolled patients with high stage HNSCC treated with docetaxel (T), cisplatin (P) and 5-fluorouracil (F) (ICT) followed by synchronous cisplatin and intensity modulated radiotherapy. Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) before and after two cycles of ICT was used to measure Fp and RECIST response.
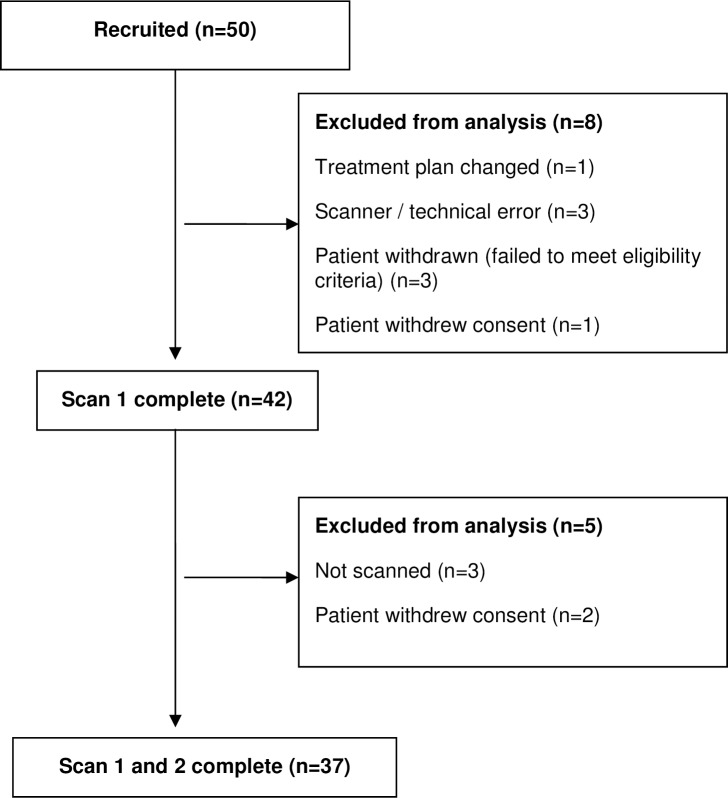
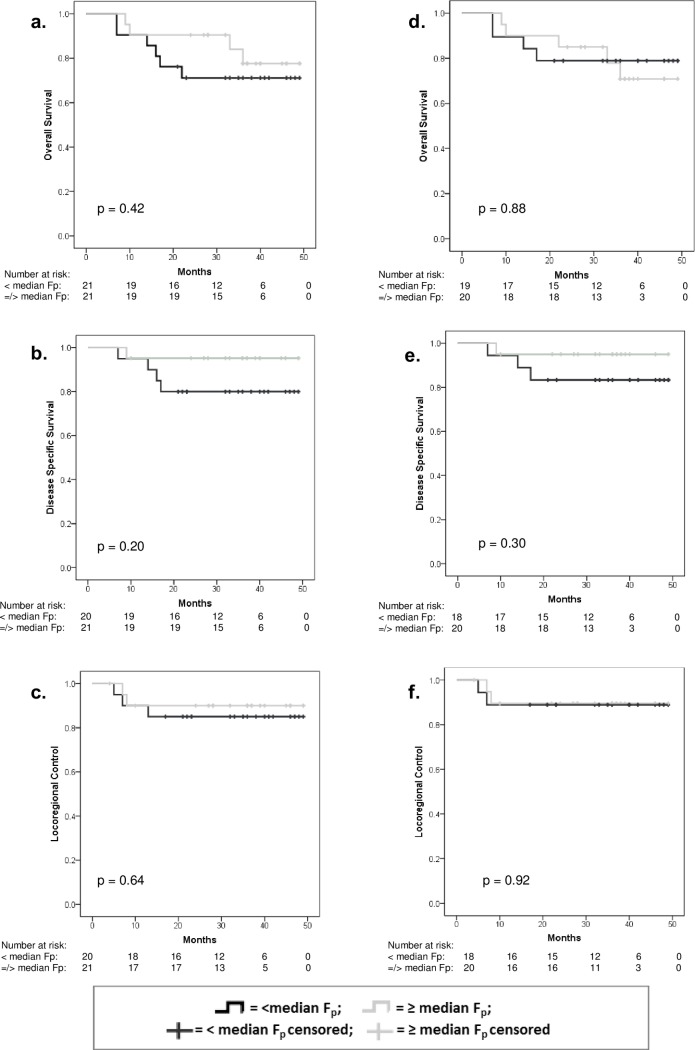
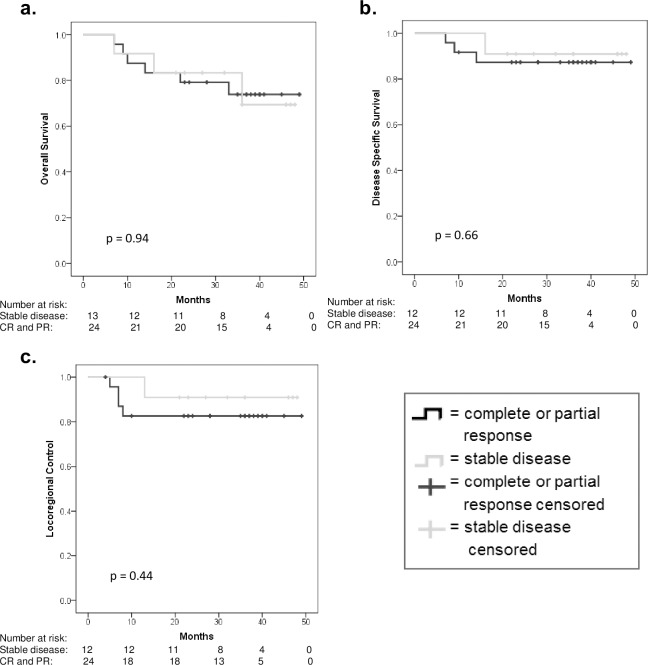
Results: Forty-two patients were recruited and 37 underwent two scans. The median follow-up was 36 (range 23-49) months. Pre-treatment tumour Fp (stratified by median) was not prognostic for overall survival (p = 0.42), disease specific survival (p = 0.20) and locoregional control (p = 0.64). Neither change in tumour Fp nor RECIST response post two cycles of ICT was prognostic for any outcome (p>0.21).
Conclusion: DCE-MRI parameters do not predict long-term survival outcomes following ICT and RECIST response to ICT may not be an appropriate endpoint to determine early efficacy of a treatment in HNSCC patients.
Conflict of interest statement
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. International Journal of Cancer. 2014:n/a-n/a. doi: 10.1002/ijc.29210 - DOI - PubMed
-
- Blanchard P, Hill C, Guihenneuc-Jouyaux C, Baey C, Bourhis J, Pignon JP. Mixed treatment comparison meta-analysis of altered fractionated radiotherapy and chemotherapy in head and neck cancer. Journal of clinical epidemiology. 2011;64(9):985–92. doi: 10.1016/j.jclinepi.2010.10.016 - DOI - PubMed
-
- Nguyen-Tan PF, Zhang Q, Ang KK, Weber RS, Rosenthal DI, Soulieres D, et al. Randomized Phase III Trial to Test Accelerated Versus Standard Fractionation in Combination With Concurrent Cisplatin for Head and Neck Carcinomas in the Radiation Therapy Oncology Group 0129 Trial: Long-Term Report of Efficacy and Toxicity. Journal of Clinical Oncology. 2014. doi: 10.1200/jco.2014.55.3925 - DOI - PMC - PubMed
-
- Bourhis J, Sire C, Graff P, Gregoire V, Maingon P, Calais G, et al. Concomitant chemoradiotherapy versus acceleration of radiotherapy with or without concomitant chemotherapy in locally advanced head and neck carcinoma (GORTEC 99–02): an open-label phase 3 randomised trial. The Lancet Oncology. 2012;13(2):145–53. Epub 2012/01/21. doi: 10.1016/S1470-2045(11)70346-1 . - DOI - PubMed
-
- Pignon J-P, Maître Al, Maillard E, Bourhis J. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiotherapy and Oncology. 2009;92(1):4–14. doi: 10.1016/j.radonc.2009.04.014 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
