

Clinical endpoints in the controlled human challenge model for Shigella: A call for standardization and the development of a disease severity score
- PMID: 29590182
- PMCID: PMC5874036
- DOI: 10.1371/journal.pone.0194325
Clinical endpoints in the controlled human challenge model for Shigella: A call for standardization and the development of a disease severity score
Abstract
Background: Since 1946 the controlled human infection model (CHIM) for Shigella has been used to improve understanding of disease pathogenesis, describe clinical and immunologic responses to infection and as a tool for vaccine development. As the frequency and intent for use in vaccine comparisons increases, standardization of the primary endpoint definition is necessary.
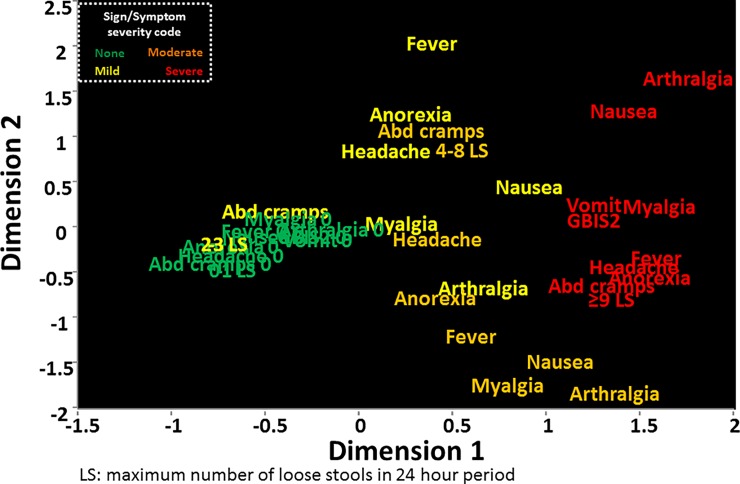
Methods: Subject-level data were obtained from previously conducted experimental Shigella CHIM studies. Signs and symptoms severity were categorized consistently across all studies. Sign and symptom correlations were estimated and univariate models were utilized to describe the association between stool output and other Shigella-attributable signs and symptoms. Multiple correspondence and hierarchical clustering analyses were performed to describe the co-occurrence of signs and symptoms. A disease score is proposed based on the co-occurrence of these events.
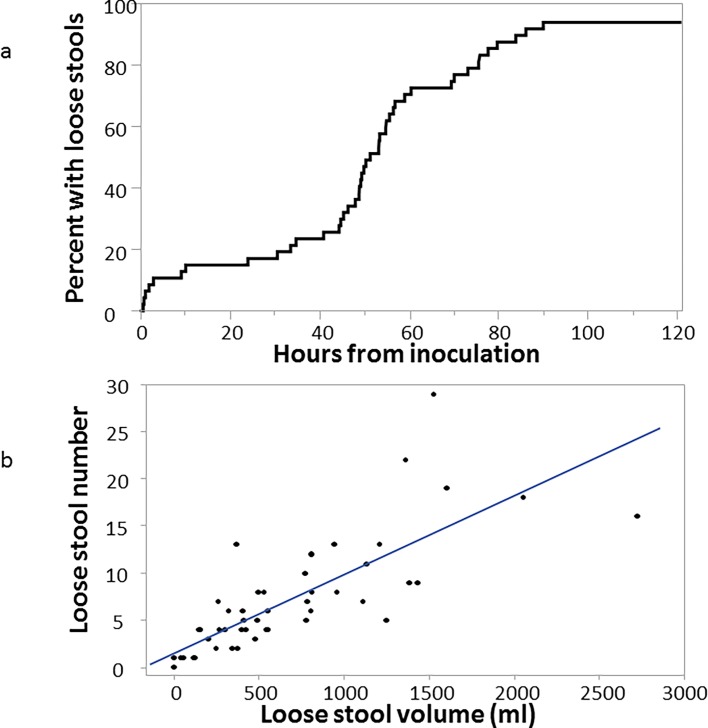
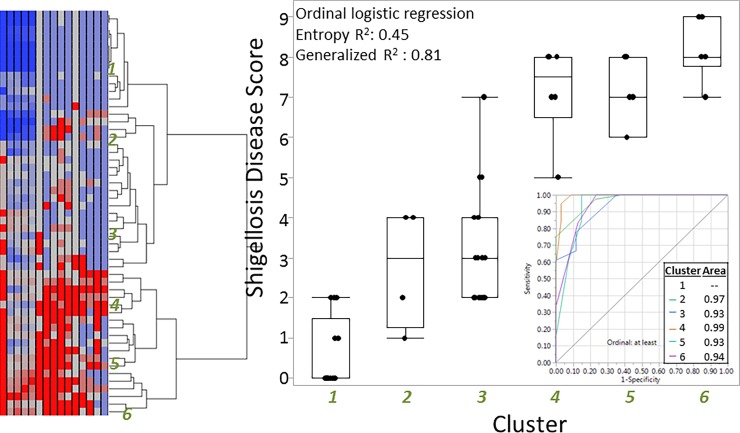
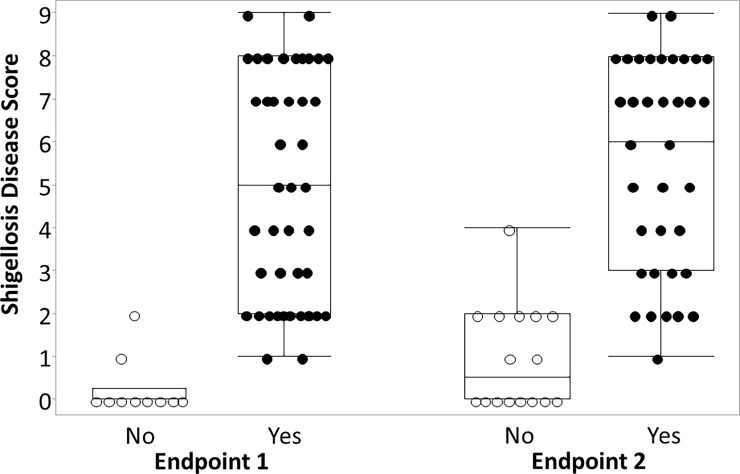
Results: Data were obtained on 54 subjects receiving 800 to 2000 colony forming units (cfu) of S. flexneri. The median maximum 24 hour stool output was 514 ml (IQR: 300, 998 ml) with a median frequency of 6 (IQR: 4, 9). Subjects reported abdominal pain or cramps (81.5%), headache (66.7%) and anorexia (64.8%), 50.0% had a fever and 27.8% had gross blood in multiple loose stools. Multiple correspondence analyses highlighted co-occurrence of symptoms based on severity. A 3-parameter disease severity score predicted shigellosis endpoints and better differentiated disease spectrum.
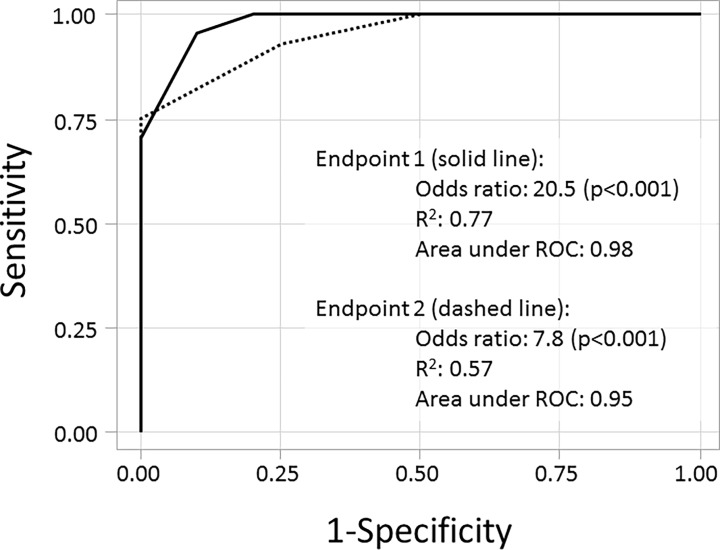
Conclusion: Dichotomous endpoints for Shigella CHIM fail to fully account for disease variability. An ordinal disease score characterizing the breadth of disease severity may enable a better characterization of shigellosis and can decrease sample size requirements. Furthermore, the disease severity score may be a useful tool for portfolio management by enabling prioritization across vaccine candidates with comparable efficacy estimates using dichotomous endpoints.
Conflict of interest statement
Figures
References
-
- Kotloff KL, Platts-Mills JA, Nasrin D, Roose A, Blackwelder WC, Levine MM. Global burden of diarrheal diseases among children in developing countries: Incidence, etiology, and insights from new molecular diagnostic techniques. Vaccine. 2017;35(49 Pt A):6783–9. 10.1016/j.vaccine.2017.07.036 . - DOI - PubMed
-
- Shah N, DuPont HL, Ramsey DJ. Global etiology of travelers' diarrhea: systematic review from 1973 to the present. Am J Trop Med Hyg. 2009;80(4):609–14. Epub 2009/04/07. doi: 80/4/609 [pii]. . - PubMed
-
- Riddle MS, Sanders JW, Putnam SD, Tribble DR. Incidence, etiology, and impact of diarrhea among long-term travelers (U.S. military and similar populations): A systematic review. Am J Trop Med Hyg. 2006;74(5):891–900. - PubMed
-
- Porter CK, Olson S, Hall A, Riddle MS. Travelers' Diarrhea: An Update on the Incidence, Etiology, and Risk in Military Deployments and Similar Travel Populations. Mil Med. 2017;182(S2):4–10. 10.7205/MILMED-D-17-00064 . - DOI - PubMed
-
- Riddle MS, Sanders JW, Putnam SD, Tribble DR. Incidence, etiology, and impact of diarrhea among long-term travelers (US military and similar populations): a systematic review. The American journal of tropical medicine and hygiene. 2006;74(5):891–900. . - PubMed
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
