

Overview of systematic reviews assessing the evidence for shorter versus longer duration antibiotic treatment for bacterial infections in secondary care
- PMID: 29590188
- PMCID: PMC5874047
- DOI: 10.1371/journal.pone.0194858
Overview of systematic reviews assessing the evidence for shorter versus longer duration antibiotic treatment for bacterial infections in secondary care
Abstract
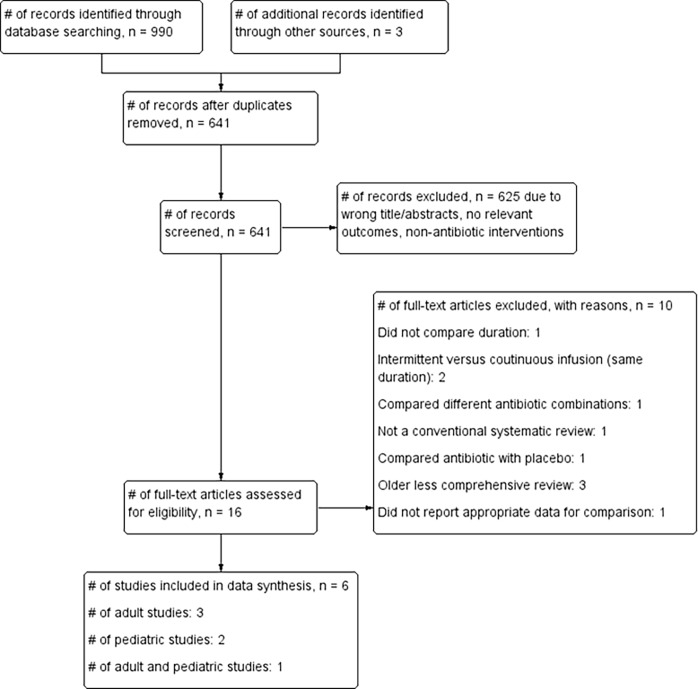
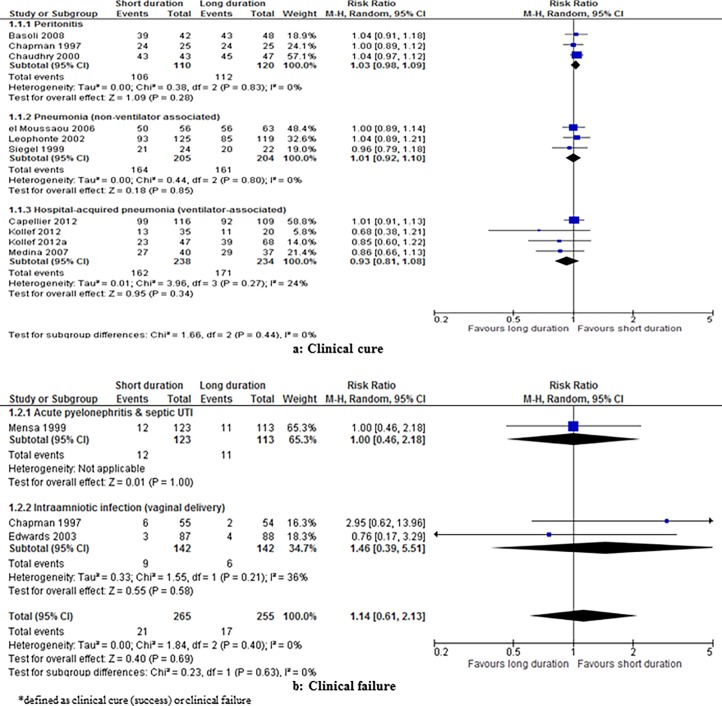
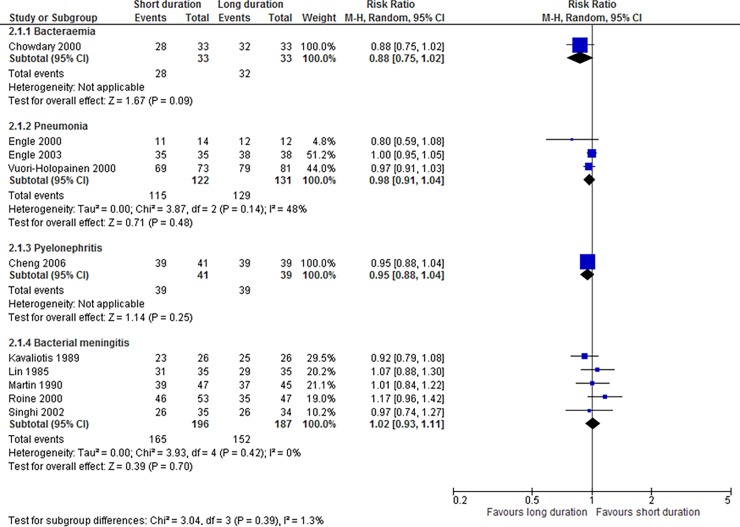
Our objective was to assess the clinical effectiveness of shorter versus longer duration antibiotics for treatment of bacterial infections in adults and children in secondary care settings, using the evidence from published systematic reviews. We conducted electronic searches in MEDLINE, Embase, Cochrane, and Cinahl. Our primary outcome was clinical resolution. The quality of included reviews was assessed using the AMSTAR criteria, and the quality of the evidence was rated using the GRADE criteria. We included 6 systematic reviews (n = 3,162). Four reviews were rated high quality, and two of moderate quality. In adults, there was no difference between shorter versus longer duration in clinical resolution rates for peritonitis (RR 1.03, 95% CI 0.98 to 1.09, I2 = 0%), ventilator-associated pneumonia (RR 0.93; 95% CI 0.81 to 1.08, I2 = 24%), or acute pyelonephritis and septic UTI (clinical failure: RR 1.00, 95% CI 0.46 to 2.18). The quality of the evidence was very low to moderate. In children, there was no difference in clinical resolution rates for pneumonia (RR 0.98, 95% CI 0.91 to 1.04, I2 = 48%), pyelonephritis (RR 0.95, 95% CI 0.88 to 1.04) and confirmed bacterial meningitis (RR 1.02, 95% CI 0.93 to 1.11, I2 = 0%). The quality of the evidence was low to moderate. In conclusion, there is currently a limited body of evidence to clearly assess the clinical benefits of shorter versus longer duration antibiotics in secondary care. High quality trials assessing strategies to shorten antibiotic treatment duration for bacterial infections in secondary care settings should now be a priority.
Conflict of interest statement
Figures
References
-
- Department of Health. UK five year antimicrobial resistance strategy 2013–2018. September 2013.
-
- World Health Organisation. The evolving threat of antimicrobial resistance—Options for action 2012. http://apps.who.int/iris/bitstream/10665/44812/1/9789241503181_eng.pdf [Last accessed 24th January, 2017].
-
- European Centre for Disease Prevention and Control. Antimicrobial resistance surveillance in Europe. Annual report of the European Antimicrobial Resistance Surveillance Network (EARS-Net) 2012, 2013.
-
- Fantin B, Duval X, Massias L, Alavoine L, Chau F, Retout S, et al. Ciprofloxacin dosage and emergence of resistance in human commensal bacteria. J Infect Dis. 2009. August 1;200(3):390–8. doi: 10.1086/600122 - DOI - PMC - PubMed
-
- Chung A, Perera R, Brueggemann AB, Elamin AE, Harnden A, Mayon-White R, et al. Effect of antibiotic prescribing on antibiotic resistance in individual children in primary care: prospective cohort study. BMJ. 2007. September 1;335(7617):429 doi: 10.1136/bmj.39274.647465.BE - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
