

Migraine and the risk of cardiovascular and cerebrovascular events: a meta-analysis of 16 cohort studies including 1 152 407 subjects
- PMID: 29593023
- PMCID: PMC5875642
- DOI: 10.1136/bmjopen-2017-020498
Migraine and the risk of cardiovascular and cerebrovascular events: a meta-analysis of 16 cohort studies including 1 152 407 subjects
Abstract
Objectives: To perform an updated meta-analysis to evaluate the long-term cardiovascular and cerebrovascular outcomes among migraineurs.
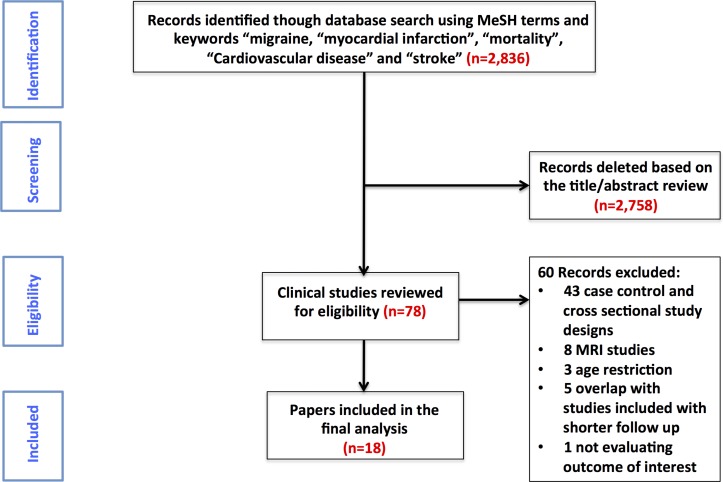
Setting: A meta-analysis of cohort studies performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Data sources: The MEDLINE, Web of Science and Cochrane Central Register of Controlled Trials databases were searched for relevant articles.
Participants: A total of 16 cohort studies (18 study records) with 394 942 migraineurs and 757 465 non-migraineurs were analysed.
Primary and secondary outcome measures: Major adverse cardiovascular and cerebrovascular events (MACCE), stroke (ie, ischaemic, haemorrhagic or non-specified), myocardial infarction (MI) and all-cause mortality. The outcomes were reported at the longest available follow-up.
Data analysis: Summary-adjusted hazard ratios (HR) were calculated by random-effects Der-Simonian and Liard model. The risk of bias was assessed by the Newcastle-Ottawa Scale.
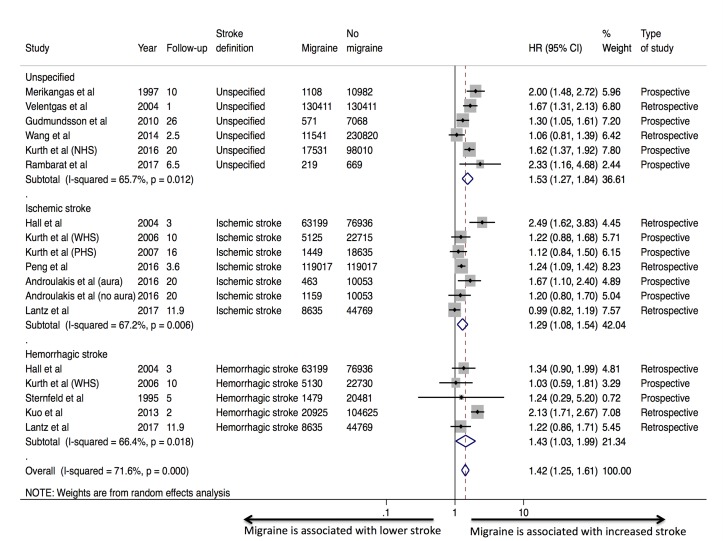
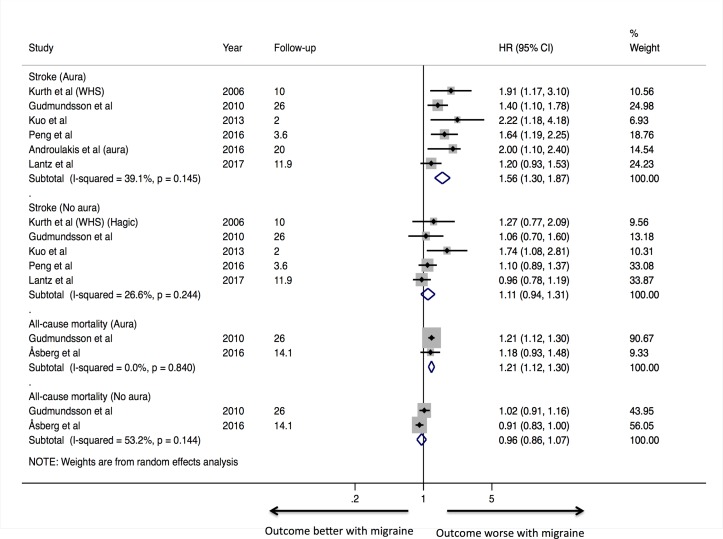
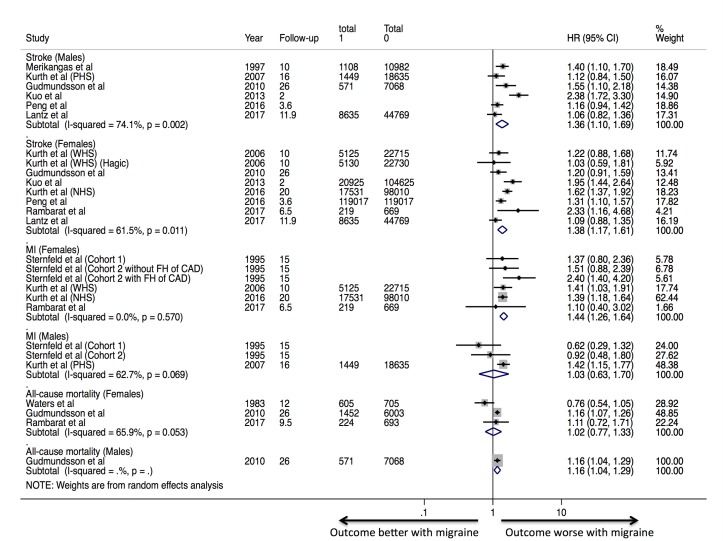
Results: Migraine was associated with a higher risk of MACCE (adjusted HR 1.42, 95% confidence interval [CI] 1.26 to 1.60, P<0.001, I2=40%) driven by a higher risk of stroke (adjusted HR 1.41, 95% CI 1.25 to 1.61, P<0.001, I2=72%) and MI (adjusted HR 1.23, 95% CI 1.03 to 1.43, P=0.006, I2=59%). There was no difference in the risk of all-cause mortality (adjusted HR 0.93, 95% CI 0.78 to 1.10, P=0.38, I2=91%), with a considerable degree of statistical heterogeneity between the studies. The presence of aura was an effect modifier for stroke (adjusted HR aura 1.56, 95% CI 1.30 to 1.87 vs adjusted HR no aura 1.11, 95% CI 0.94 to 1.31, P interaction=0.01) and all-cause mortality (adjusted HR aura 1.20, 95% CI 1.12 to 1.30 vs adjusted HR no aura 0.96, 95% CI 0.86 to 1.07, Pinteraction<0.001).
Conclusion: Migraine headache was associated with an increased long-term risk of cardiovascular and cerebrovascular events. This effect was due to an increased risk of stroke (both ischaemic and haemorrhagic) and MI. There was a moderate to severe degree of heterogeneity for the outcomes, which was partly explained by the presence of aura.
Prospero registration number: CRD42016052460.
Keywords: cardiac epidemiology; migraine; myocardial infarction; stroke.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous