

The British Society of Gastroenterology/UK-PBC primary biliary cholangitis treatment and management guidelines
- PMID: 29593060
- PMCID: PMC6109281
- DOI: 10.1136/gutjnl-2017-315259
The British Society of Gastroenterology/UK-PBC primary biliary cholangitis treatment and management guidelines
Abstract
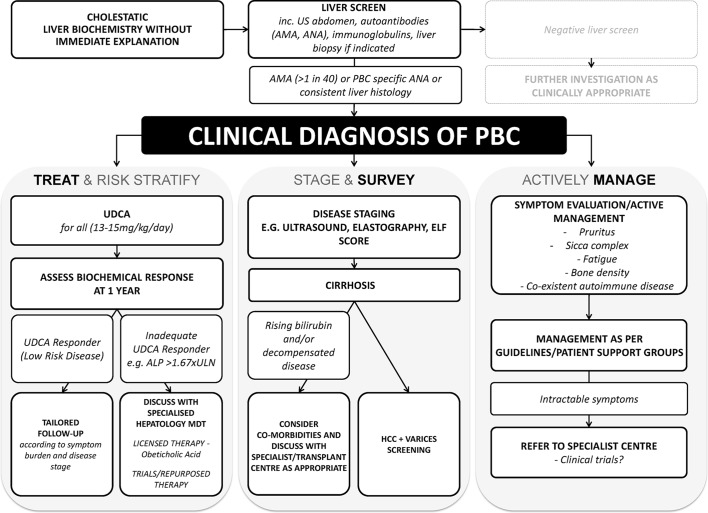
Primary biliary cholangitis (formerly known as primary biliary cirrhosis, PBC) is an autoimmune liver disease in which a cycle of immune mediated biliary epithelial cell injury, cholestasis and progressive fibrosis can culminate over time in an end-stage biliary cirrhosis. Both genetic and environmental influences are presumed relevant to disease initiation. PBC is most prevalent in women and those over the age of 50, but a spectrum of disease is recognised in adult patients globally; male sex, younger age at onset (<45) and advanced disease at presentation are baseline predictors of poorer outcome. As the disease is increasingly diagnosed through the combination of cholestatic serum liver tests and the presence of antimitochondrial antibodies, most presenting patients are not cirrhotic and the term cholangitis is more accurate. Disease course is frequently accompanied by symptoms that can be burdensome for patients, and management of patients with PBC must address, in a life-long manner, both disease progression and symptom burden. Licensed therapies include ursodeoxycholic acid (UDCA) and obeticholic acid (OCA), alongside experimental new and re-purposed agents. Disease management focuses on initiation of UDCA for all patients and risk stratification based on baseline and on-treatment factors, including in particular the response to treatment. Those intolerant of treatment with UDCA or those with high-risk disease as evidenced by UDCA treatment failure (frequently reflected in trial and clinical practice as an alkaline phosphatase >1.67 × upper limit of normal and/or elevated bilirubin) should be considered for second-line therapy, of which OCA is the only currently licensed National Institute for Health and Care Excellence recommended agent. Follow-up of patients is life-long and must address treatment of the disease and management of associated symptoms.
Keywords: autoimmune liver disease; care pathway; guidelines; obeticholic acid; ursodeoxycholic acid.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: GMH: Advisory boards for Falk, GfK, GSK, Intercept, Novartis; consultancy for CymaBay; clinical trial investigator for Falk, FF Pharma, Gilead, GSK, Intercept, Novartis, NGM Bio, Shire. JKD: member of BSG and BASL. GJMA: department receives/received financial support for clinical trials from GSK, Intercept and Cymabay. IP: honorarium received for chairing sessions/lectures/meetings and sponsorship to attend Falk Symposium from Dr Falk Pharma. DT: department receives/received financial support for hosting and speaking at meetings from Dr Falk Pharma. MW: holds a voluntary position as the chair of Trustees for PSC Support. DEJJ: grant funding from Pfizer and Intercept; consultancy for Intercept, GSK and Novartis; speaker bureau for Dr Falk Pharma. Member of medical advisory board for PBC Foundation.
Figures
Comment in
-
Antipruritic effect of bezafibrate and serum autotaxin measures in patients with primary biliary cholangitis.Gut. 2019 Oct;68(10):1902-1903. doi: 10.1136/gutjnl-2018-317426. Epub 2018 Sep 18. Gut. 2019. PMID: 30228218 No abstract available.
Similar articles
-
Obeticholic acid for the treatment of primary biliary cholangitis.Expert Opin Pharmacother. 2016 Sep;17(13):1809-15. doi: 10.1080/14656566.2016.1218471. Epub 2016 Aug 9. Expert Opin Pharmacother. 2016. PMID: 27468093 Review.
-
Primary Biliary Cholangitis: Medical and Specialty Pharmacy Management Update.J Manag Care Spec Pharm. 2016 Oct;22(10-a-s Suppl):S3-S15. doi: 10.18553/jmcp.2016.22.10-a-s.s3. J Manag Care Spec Pharm. 2016. PMID: 27700211 Free PMC article. Review.
-
Pretreatment prediction of response to ursodeoxycholic acid in primary biliary cholangitis: development and validation of the UDCA Response Score.Lancet Gastroenterol Hepatol. 2018 Sep;3(9):626-634. doi: 10.1016/S2468-1253(18)30163-8. Epub 2018 Jul 13. Lancet Gastroenterol Hepatol. 2018. PMID: 30017646 Free PMC article.
-
Longitudinal outcomes of obeticholic acid therapy in ursodiol-nonresponsive primary biliary cholangitis: Stratifying the impact of add-on fibrates in real-world practice.Aliment Pharmacol Ther. 2024 Jun;59(12):1604-1615. doi: 10.1111/apt.18004. Epub 2024 May 1. Aliment Pharmacol Ther. 2024. PMID: 38690746
-
Management of primary biliary cholangitis prior to obeticholic acid availability.Minerva Med. 2018 Dec;109(6):410-417. doi: 10.23736/S0026-4806.18.05774-9. Epub 2018 Jul 18. Minerva Med. 2018. PMID: 30022645
Cited by
-
Role of ductular reaction and ductular-canalicular junctions in identifying severe primary biliary cholangitis.JHEP Rep. 2022 Aug 19;4(11):100556. doi: 10.1016/j.jhepr.2022.100556. eCollection 2022 Nov. JHEP Rep. 2022. PMID: 36267871 Free PMC article.
-
Accuracy of Transient Elastography in Assessing Fibrosis at Diagnosis in Naïve Patients With Primary Biliary Cholangitis: A Dual Cut-Off Approach.Hepatology. 2021 Sep;74(3):1496-1508. doi: 10.1002/hep.31810. Epub 2021 May 28. Hepatology. 2021. PMID: 33724515 Free PMC article.
-
Rare renal proximal tubular dysfunctions in primary biliary cholangitis.Ren Fail. 2024 Dec;46(1):2302409. doi: 10.1080/0886022X.2024.2302409. Epub 2024 Jan 26. Ren Fail. 2024. PMID: 38275162 Free PMC article.
-
The Evolving Use of Biochemical Markers in the Management of Primary Biliary Cholangitis: Discussion.Gastroenterol Hepatol (N Y). 2021 May;17(5 Suppl 5):14-17. Gastroenterol Hepatol (N Y). 2021. PMID: 34135722 Free PMC article. No abstract available.
-
Home-based exercise in patients with refractory fatigue associated with primary biliary cholangitis: a protocol for the EXerCise Intervention in cholesTatic LivEr Disease (EXCITED) feasibility trial.BMJ Open Gastroenterol. 2021 Mar;8(1):e000579. doi: 10.1136/bmjgast-2020-000579. BMJ Open Gastroenterol. 2021. PMID: 33707216 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials