

Acute Hemorrhagic Encephalitis Responding to Combined Decompressive Craniectomy, Intravenous Immunoglobulin, and Corticosteroid Therapies: Association with Novel RANBP2 Variant
- PMID: 29593631
- PMCID: PMC5857578
- DOI: 10.3389/fneur.2018.00130
Acute Hemorrhagic Encephalitis Responding to Combined Decompressive Craniectomy, Intravenous Immunoglobulin, and Corticosteroid Therapies: Association with Novel RANBP2 Variant
Abstract
Background: Acute hemorrhagic encephalomyelitis (AHEM) is considered as a rare form of acute disseminated encephalomyelitis characterized by fulminant encephalopathy with hemorrhagic necrosis and most often fatal outcome.
Objective: To report the association with Ran Binding Protein (RANBP2) gene variant and the response to decompressive craniectomy and high-dose intravenous methylprednisolone (IVMP) in life-threatening AHEM.
Design: Single case study.
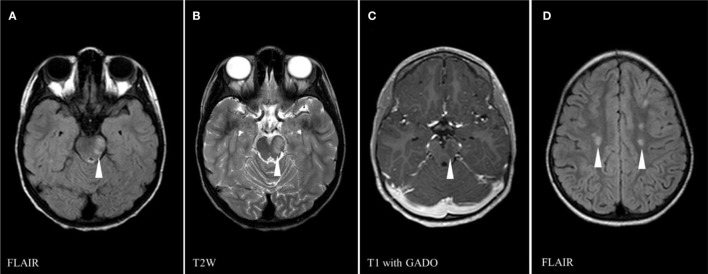
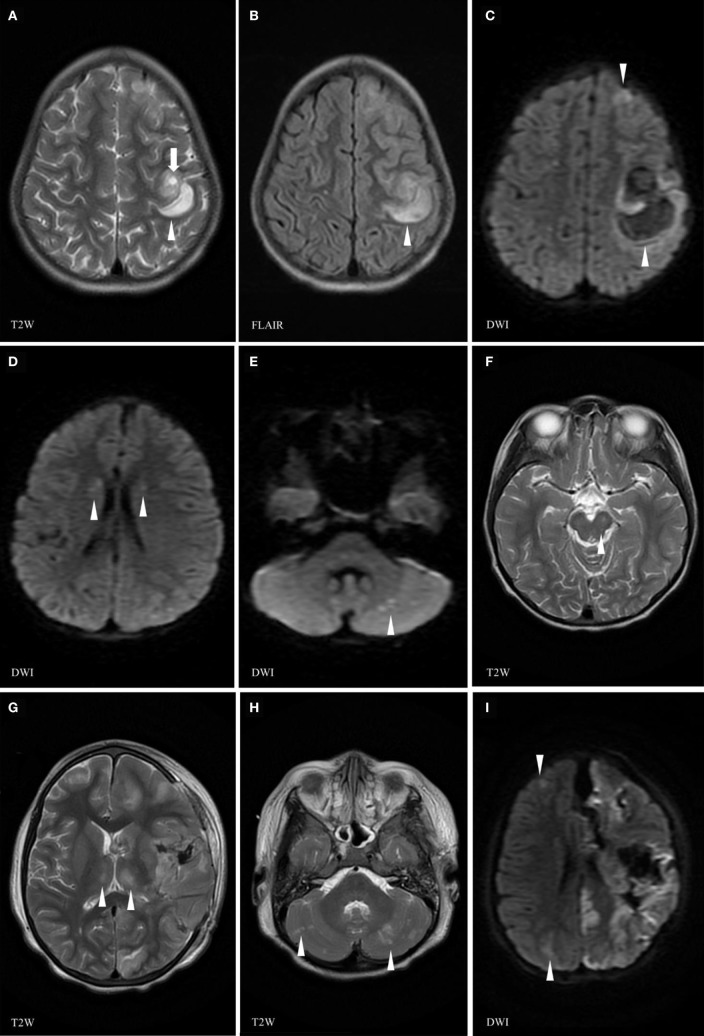
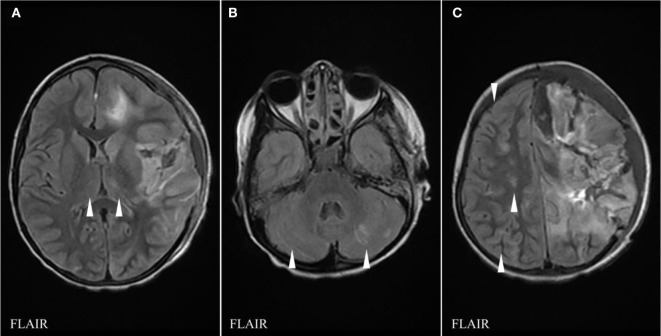
Case report: A 6-year-old girl known to have sickle cell disease (SCD) presented an acquired demyelinating syndrome (ADS) with diplopia due to sudden unilateral fourth nerve palsy. She received five pulses of IVMP (30 mg/kg/day). Two weeks after steroid weaning, she developed right hemiplegia and coma. Brain magnetic resonance imaging showed a left frontal necrotico-hemorrhagic lesion and new multifocal areas of demyelination. She underwent decompressive craniotomy and evacuation of an ongoing left frontoparietal hemorrhage. Comprehensive investigations ruled out vascular and infectious process. The neurological deterioration stopped concomitantly with combined neurosurgical drainage of the hematoma, decompressive craniotomy, IVMP, and intravenous immunoglobulins (IVIG). She developed during the following months Crohn disease and sclerosing cholangitis. After 2-year follow-up, there was no new neurological manifestation. The patient still suffered right hemiplegia and aphasia, but was able to walk. Cognitive/behavioral abilities significantly recovered. A heterozygous novel rare missense variant (c.4993A>G, p.Lys1665Glu) was identified in RANBP2, a gene associated with acute necrotizing encephalopathy. RANBP2 is a protein playing an important role in the energy homeostasis of neuronal cells.
Conclusion: In any ADS occurring in the context of SCD and/or autoimmune condition, we recommend to slowly wean steroids and to closely monitor the patient after weaning to quickly treat any recurrence of neurological symptom with IVMP. This case report, in addition to others, stresses the likely efficacy of combined craniotomy, IVIG, and IVMP treatments in AHEM. RANBP2 mutations may sensitize the brain to inflammation and predispose to AHEM.
Keywords: Acute demyelinating encephalomyelitis; Acute necrotizing encephalopathy; Crohn disease; RANBP2; encephalitis; sclerosing cholangitis; sickle cell disease.
Figures
Similar articles
-
Recurrent acute necrotizing encephalopathy in a boy with RANBP2 mutation and thermolabile CPT2 variant: The first case of ANE1 in Japan.Brain Dev. 2021 Sep;43(8):873-878. doi: 10.1016/j.braindev.2021.04.009. Epub 2021 May 28. Brain Dev. 2021. PMID: 34059398
-
Familial acute necrotizing encephalopathy with RANBP2 mutation: The first report in Northeast Asia.Brain Dev. 2017 Aug;39(7):625-628. doi: 10.1016/j.braindev.2017.02.005. Epub 2017 Mar 21. Brain Dev. 2017. PMID: 28336122 Free PMC article.
-
Acute necrotizing encephalopathy associated with RANBP2 mutation: value of MRI findings for diagnosis and intervention.Acta Neurol Belg. 2023 Apr;123(2):571-582. doi: 10.1007/s13760-022-02166-x. Epub 2022 Dec 26. Acta Neurol Belg. 2023. PMID: 36572756 Free PMC article.
-
Acute haemorrhagic leukoencephalitis (AHLE) - our experience and a short review.J Neuroimmunol. 2021 Dec 15;361:577751. doi: 10.1016/j.jneuroim.2021.577751. Epub 2021 Oct 13. J Neuroimmunol. 2021. PMID: 34739912 Review.
-
RANBP2 mutation and acute necrotizing encephalopathy: 2 cases and a literature review of the expanding clinico-radiological phenotype.Eur J Paediatr Neurol. 2015 Mar;19(2):106-13. doi: 10.1016/j.ejpn.2014.11.010. Epub 2014 Dec 9. Eur J Paediatr Neurol. 2015. PMID: 25522933 Review.
Cited by
-
Fatal Acute Hemorrhagic Leukoencephalitis Following Immunization Against Human Papillomavirus in a 14-Year-Old Boy.Child Neurol Open. 2021 May 18;8:2329048X211016109. doi: 10.1177/2329048X211016109. eCollection 2021 Jan-Dec. Child Neurol Open. 2021. PMID: 34046515 Free PMC article.
-
Clinical Manifestations and Pathogenesis of Acute Necrotizing Encephalopathy: The Interface Between Systemic Infection and Neurologic Injury.Front Neurol. 2022 Jan 4;12:628811. doi: 10.3389/fneur.2021.628811. eCollection 2021. Front Neurol. 2022. PMID: 35058867 Free PMC article. Review.
-
Increased Intracranial Pressure in Pediatric Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease.Neurol Neuroimmunol Neuroinflamm. 2023 Nov 2;11(1):e200174. doi: 10.1212/NXI.0000000000200174. Print 2024 Jan. Neurol Neuroimmunol Neuroinflamm. 2023. PMID: 37918972 Free PMC article.
-
MicroRNAs miR-451a and Let-7i-5p Profiles in Circulating Exosomes Vary among Individuals with Different Sickle Hemoglobin Genotypes and Malaria.J Clin Med. 2022 Jan 19;11(3):500. doi: 10.3390/jcm11030500. J Clin Med. 2022. PMID: 35159951 Free PMC article.
-
Clinical use of steroids in viral central nervous system (CNS) infections: three challenging cases.J Neurovirol. 2021 Oct;27(5):727-734. doi: 10.1007/s13365-021-01008-5. Epub 2021 Oct 1. J Neurovirol. 2021. PMID: 34596868
References
-
- Hurst EW. Acute hemorrhagic leukoencephalitis: a previously undefined entity. Med J Aust (1941) 2:1–6.
-
- Adams RD, Cammermeyer J, Dennybrown D. Acute necrotizing hemorrhagic encephalopathy. J Neuropathol Exp Neurol (1948) 7(1):111. - PubMed
-
- Byers RK. Acute hemorrhagic leukoencephalitis: report of three cases and review of the literature. Pediatrics (1975) 56(5):727–35. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous