

Hypophysitis following Treatment with Ustekinumab: Radiological and Pathological Findings
- PMID: 29593650
- PMCID: PMC5854641
- DOI: 10.3389/fendo.2018.00083
Hypophysitis following Treatment with Ustekinumab: Radiological and Pathological Findings
Abstract
Context: Ustekinumab is a human IgG1 monoclonal antibody that targets interleukin (IL)-12 and IL-23, which may be useful in the treatment of autoimmune conditions such as psoriasis, psoriatic arthritis, and Crohn's disease. Hypophysitis is an immune-derived inflammatory condition of the pituitary gland that may lead to pituitary dysfunction. With the increasing use of immunotherapy, it is possible that this and other new immune-related adverse events (IRAEs) arise, although the mechanisms involved are still incompletely defined.
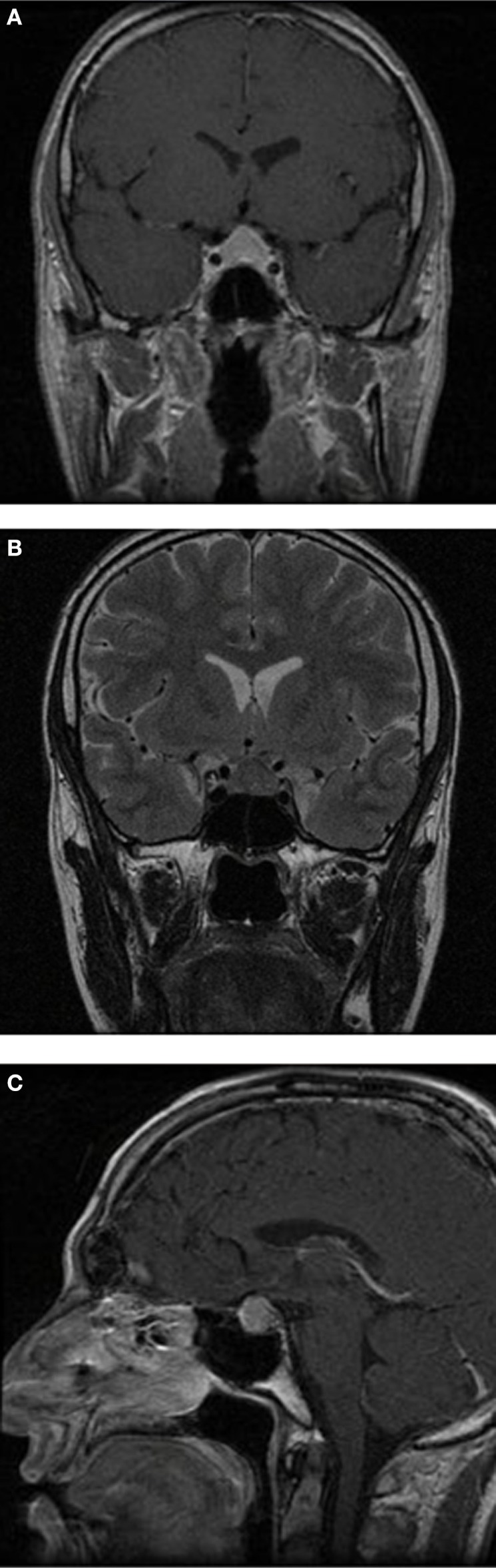
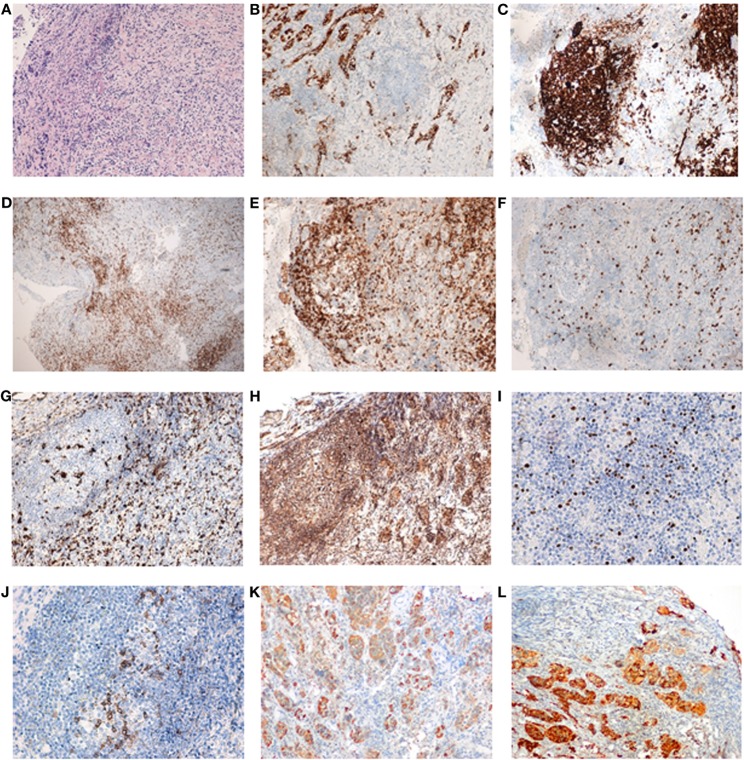
Case description: A 35-year-old male, with a previous history of severe plaque-psoriasis who had started treatment with ustekinumab 4 months before, complained of progressive and persistent headache. Brain magnetic resonance imaging (MRI) was unremarkable. One year later, a new MRI was performed due to headache persistence, which revealed a homogenous and diffuse pituitary enlargement, with suprasellar extension and optic chiasm involvement, blurring of the pituitary stalk, absence of clear differentiation between the anterior and posterior lobes, and no signs of hemorrhage or adenomas. Endocrine evaluation was consistent with panhypopituitarism. Work-up of infiltrative and infectious diseases was negative. Follow-up MRI revealed an increase in the pituitary enlargement and transsphenoidal surgery was performed. Pathological findings revealed an intense fibrosis and a chronic inflammatory infiltrate, but no evidence of adenoma, granuloma, or acid fast bacilli. Immunohistochemical staining showed a combined T-cell (CD3+, CD4+) and B-cell (CD19+, CD20+) phenotype.
Conclusion: We suggest a novel IRAE of ustekinumab, with full radiological and immunopathological iconography, which may be mediated by the complex interaction between different immunological processes.
Keywords: autoimmunity; hypophysitis; pituitary; psoriasis; ustekinumab.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials