

Bioprosthetic Valve Fracture During Valve-in-valve TAVR: Bench to Bedside
- PMID: 29593832
- PMCID: PMC5872348
- DOI: 10.15420/icr.2017:29:1
Bioprosthetic Valve Fracture During Valve-in-valve TAVR: Bench to Bedside
Abstract
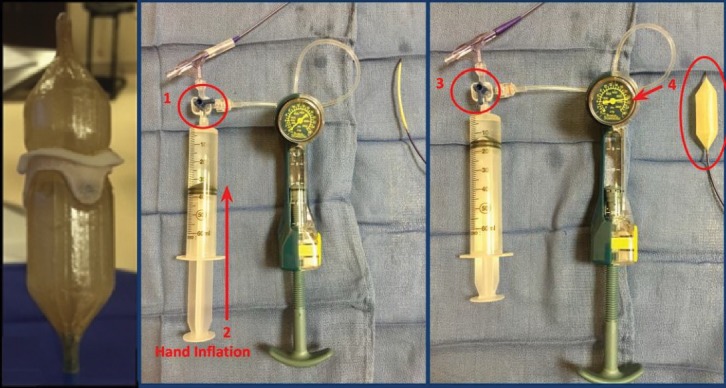
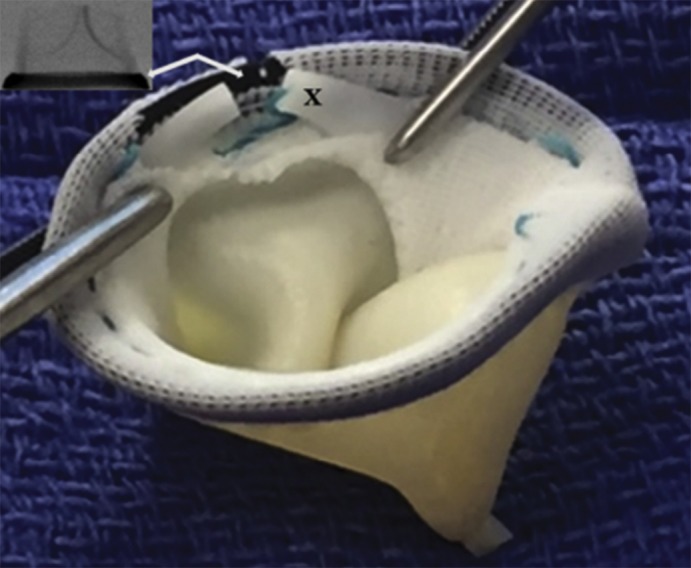
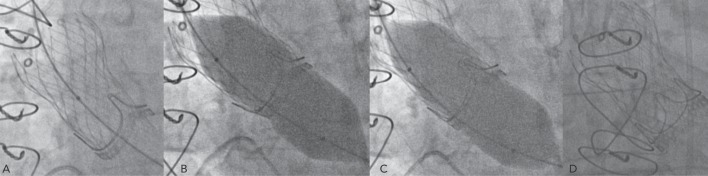
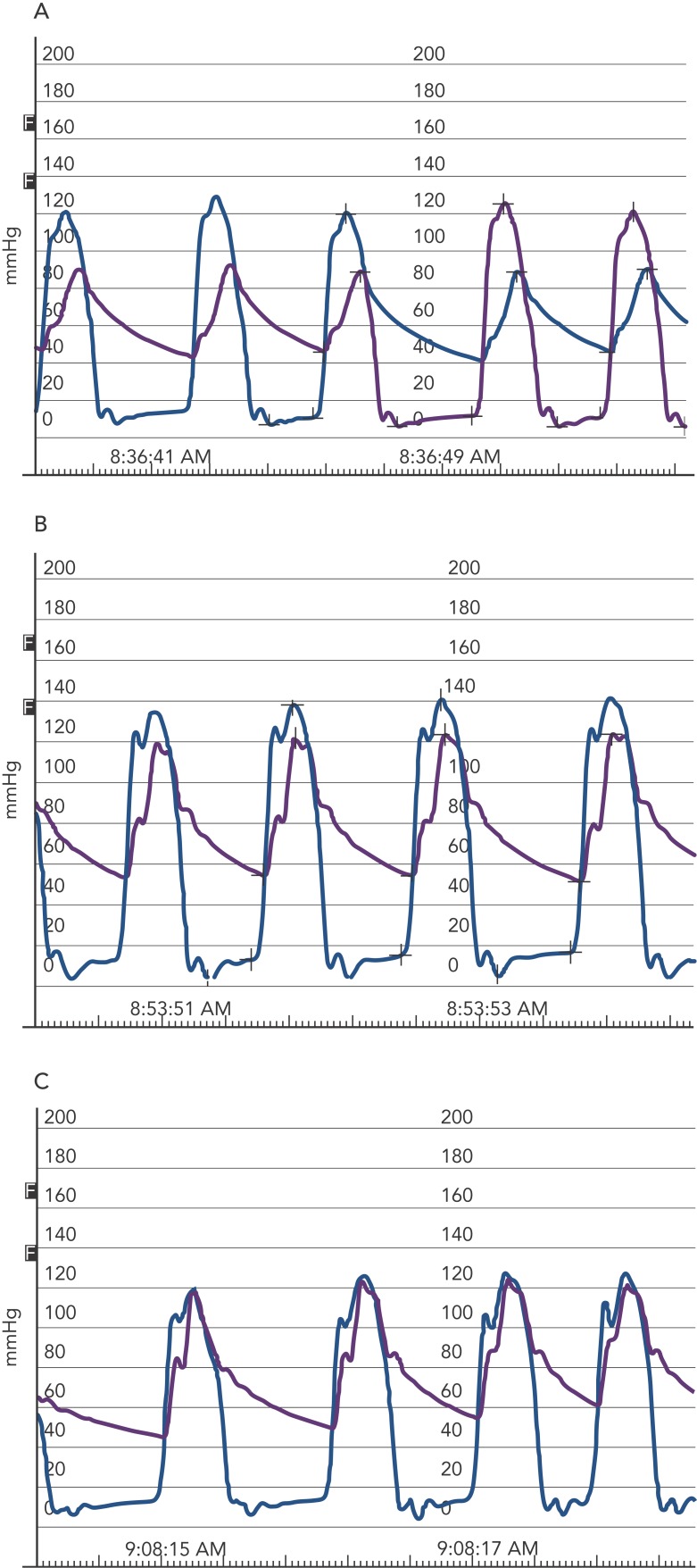
Valve-in-valve (VIV) transcatheter aortic valve replacement (TAVR) has been established as a safe and effective means of treating failed surgical bioprosthetic valves (BPVs) in patients at high risk for complications related to reoperation. Patients who undergo VIV TAVR are at risk of patient-prosthesis mismatch, as the transcatheter heart valve (THV) is implanted within the ring of the existing BPV, limiting full expansion and reducing the maximum achievable effective orifice area of the THV. Importantly, patient-prosthesis mismatch and high residual transvalvular gradients are associated with reduced survival following VIV TAVR. Bioprosthetic valve fracture (BVF) is as a novel technique to address this problem. During BPV, a non-compliant valvuloplasty balloon is positioned within the BPV frame, and a highpressure balloon inflation is performed to fracture the surgical sewing ring of the BPV. This allows for further expansion of the BPV as well as the implanted THV, thus increasing the maximum effective orifice area that can be achieved after VIV TAVR. This review focuses on the current evidence base for BVF to facilitate VIV TAVR, including initial bench testing, procedural technique, clinical experience and future directions.
Keywords: Transcatheter aortic valve replacement; aortic stenosis; bioprosthetic valve fracture; patient–prosthesis mismatch; valve-in-valve TAVR.
Conflict of interest statement
Disclosure: Dr. Chhatriwalla receives research and clinical trial support from, acts as a proctor of, and is on the speakers bureau of Medtronic, Edwards Lifesciences and St. Jude Medical. Dr. Cohen receives research and clinical trial support from Medtronic, St. Jude Medical, and Edwards Lifesciences. Dr. Allen receives research support from Abbott Medical and Edwards Lifesciences, and is on the speakers bureau of Edwards Lifesciences and Medtronic. Dr. Saxon has no disclosures.
Figures
Similar articles
-
Valve-in-Valve Transcatheter Aortic Valve Replacement and Bioprosthetic Valve Fracture Comparing Different Transcatheter Heart Valve Designs: An Ex Vivo Bench Study.JACC Cardiovasc Interv. 2019 Jan 14;12(1):65-75. doi: 10.1016/j.jcin.2018.10.043. JACC Cardiovasc Interv. 2019. PMID: 30621980
-
Bioprosthetic Valve Fracture Improves the Hemodynamic Results of Valve-in-Valve Transcatheter Aortic Valve Replacement.Circ Cardiovasc Interv. 2017 Jul;10(7):e005216. doi: 10.1161/CIRCINTERVENTIONS.117.005216. Circ Cardiovasc Interv. 2017. PMID: 28698291
-
Bioprosthetic valve fracture: a practical guide.Ann Cardiothorac Surg. 2021 Sep;10(5):564-570. doi: 10.21037/acs-2021-tviv-25. Ann Cardiothorac Surg. 2021. PMID: 34733685 Free PMC article. Review.
-
Bioprosthetic valve fracture: Technical insights from a multicenter study.J Thorac Cardiovasc Surg. 2019 Nov;158(5):1317-1328.e1. doi: 10.1016/j.jtcvs.2019.01.073. Epub 2019 Jan 31. J Thorac Cardiovasc Surg. 2019. PMID: 30857820
-
Is Bioprosthetic Valve Fracture Beneficial for Patients with Larger Surgical Valves Undergoing Valve in Valve TAVR?Curr Cardiol Rep. 2018 Aug 22;20(10):95. doi: 10.1007/s11886-018-1035-2. Curr Cardiol Rep. 2018. PMID: 30135999 Review.
Cited by
-
Unusual cause of severe transvalvular eccentric jet AR: early structure valve deterioration of Trifecta valves by flail leaflet undergoing valve-in-valve transcatheter aortic valve replacement.BMJ Case Rep. 2024 Feb 23;17(2):e256369. doi: 10.1136/bcr-2023-256369. BMJ Case Rep. 2024. PMID: 38395470
-
Balloon Aortic Valvuloplasty in the Modern Era: A Review of Outcomes, Indications, and Technical Advances.J Soc Cardiovasc Angiogr Interv. 2023 Jul 27;2(4):101002. doi: 10.1016/j.jscai.2023.101002. eCollection 2023 Jul-Aug. J Soc Cardiovasc Angiogr Interv. 2023. PMID: 39131636 Free PMC article. Review.
-
Valve-in-Valve TAVR versus Redo Surgical Aortic Valve Replacement: Early Outcomes.Thorac Cardiovasc Surg. 2023 Mar;71(2):94-100. doi: 10.1055/s-0041-1735476. Epub 2021 Sep 14. Thorac Cardiovasc Surg. 2023. PMID: 34521136 Free PMC article.
-
Balloon Fracturing Valve-in-Valve: How to Do It and a Case Report of TAVR in a Rapid Deployment Prosthesis.J Interv Cardiol. 2022 May 4;2022:4368887. doi: 10.1155/2022/4368887. eCollection 2022. J Interv Cardiol. 2022. PMID: 35600211 Free PMC article. Review.
-
Bioprosthetic Aortic Valve Fracture During Valve-in-valve Transcatheter Aortic Valve Implantation.Interv Cardiol. 2019 Nov 18;14(3):147-151. doi: 10.15420/icr.2019.08.R2. eCollection 2019 Nov. Interv Cardiol. 2019. PMID: 31867060 Free PMC article. Review.
References
-
- Leon MB, Smith CR. Transcatheter aortic-valve replacement. N Engl J Med. 2016;375:700–1. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
