

Cancer Screening Among U.S. Medicaid Enrollees with Chronic Comorbidities or Residing in Long-Term Care Facilities
- PMID: 29593845
- PMCID: PMC5868748
- DOI: 10.6000/1927-7229.2013.02.02.6
Cancer Screening Among U.S. Medicaid Enrollees with Chronic Comorbidities or Residing in Long-Term Care Facilities
Abstract
Background: Ensuring appropriate cancer screenings among low-income persons with chronic conditions and persons residing in long-term care (LTC) facilities presents special challenges. This study examines the impact of having chronic diseases and of LTC residency status on cancer screening among adults enrolled in Medicaid, a joint state-federal government program providing health insurance for certain low-income individuals in the U.S.
Methods: We used 2000-2003 Medicaid data for Medicaid-only beneficiaries and merged 2003 Medicare-Medicaid data for dually-eligible beneficiaries from four states to estimate the likelihood of cancer screening tests during a 12-month period. Multivariate regression models assessed the association of chronic conditions and LTC residency status with each type of cancer screening.
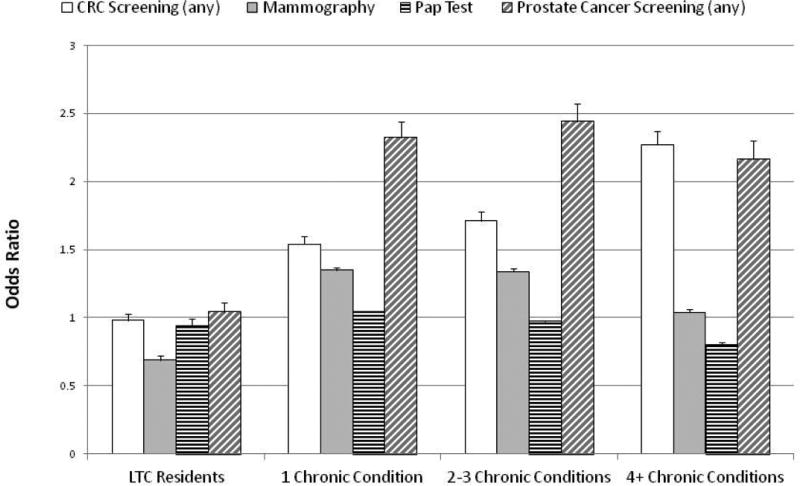
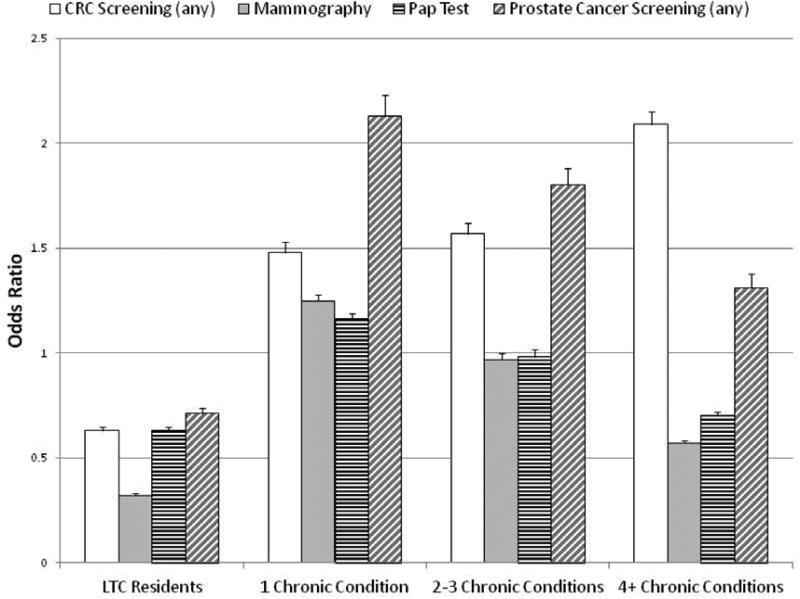
Results: LTC residency was associated with significant reductions in screening tests for both Medicaid-only and Medicare-Medicaid enrollees; particularly large reductions were observed for receipt of mammograms. Enrollees with multiple chronic comorbidities were more likely to receive colorectal and prostate cancer screenings and less likely to receive Papanicolaou (Pap) tests than were those without chronic conditions.
Conclusions: LTC residents have substantial risks of not receiving cancer screening tests. Not performing appropriate screenings may increase the risk of delayed/missed diagnoses and could increase disparities; however, it is also important to consider recommendations to appropriately discontinue screening and decrease the risk of overdiagnosis. Although anecdotal reports suggest that patients with serious comorbidities may not receive regular cancer screening, we found that having chronic conditions increases the likelihood of certain screening tests. More work is needed to better understand these issues and to facilitate referrals for appropriate cancer screenings.
Keywords: Healthcare Disparities; Mass Screening; Medicaid; Neoplasms; Nursing Homes.
Conflict of interest statement
The authors have no conflict of interest.
Figures
Similar articles
-
Cancer outcomes in low-income elders: is there an advantage to being on Medicaid?Medicare Medicaid Res Rev. 2012 Jul 30;2(2):mmrr.002.02.a06. doi: 10.5600/mmrr.002.02.a06. eCollection 2012. Medicare Medicaid Res Rev. 2012. PMID: 24800139 Free PMC article.
-
Effect of long-term care use on Medicare and Medicaid expenditures for dual eligible and non-dual eligible elderly beneficiaries.Medicare Medicaid Res Rev. 2013 Aug 22;3(3):mmrr.003.03.a05. doi: 10.5600/mmrr.003.03.a05. eCollection 2013. Medicare Medicaid Res Rev. 2013. PMID: 24753971 Free PMC article.
-
Factors Influencing Receipt of Interventional Pain Management Among Medicaid Beneficiaries with Cancer.Pain Physician. 2019 May;22(3):E147-E155. Pain Physician. 2019. PMID: 31151338
-
Quality, Spending, Utilization, and Outcomes Among Dual-Eligible Medicare-Medicaid Beneficiaries in Integrated Care Programs: A Systematic Review.JAMA Health Forum. 2024 Jul 5;5(7):e242187. doi: 10.1001/jamahealthforum.2024.2187. JAMA Health Forum. 2024. PMID: 39028653 Free PMC article.
-
Behavioral Health Conditions and Health Care Expenditures of Adults Aged 18 to 64 Dually Eligible for Medicaid and Medicare.2014 Jul 15. In: The CBHSQ Report. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2013–. 2014 Jul 15. In: The CBHSQ Report. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2013–. PMID: 27631062 Free Books & Documents. Review.
Cited by
-
Impact of state-specific Medicaid reimbursement and eligibility policies on receipt of cancer screening.Cancer. 2014 Oct 1;120(19):3016-24. doi: 10.1002/cncr.28704. Epub 2014 Aug 25. Cancer. 2014. PMID: 25154930 Free PMC article.
-
Random survival forests using linked data to measure illness burden among individuals before or after a cancer diagnosis: Development and internal validation of the SEER-CAHPS illness burden index.Int J Med Inform. 2021 Jan;145:104305. doi: 10.1016/j.ijmedinf.2020.104305. Epub 2020 Oct 21. Int J Med Inform. 2021. PMID: 33188949 Free PMC article.
References
-
- Welch HG, Black WC. Overdiagnosis in cancer. J Natl Cancer Inst. 2010;102:605–13. http://dx.doi.org/10.1093/jnci/djq099. - DOI - PubMed
-
- Castellano PZ, Wenger NK, Graves WL. Adherence to screening guidelines for breast and cervical cancer in postmenopausal women with coronary heart disease: an ancillary study of volunteers for hers. J Womens Health Gend Based Med. 2001;10:451–61. http://dx.doi.org/10.1089/152460901300233920. - DOI - PubMed
-
- Heflin MT, Pollak KI, Kuchibhatla MN, Branch LG, Oddone EZ. The impact of health status on physicians' intentions to offer cancer screening to older women. J Gerontol A Biol Sci Med Sci. 2006;61:844–50. http://dx.doi.org/10.1093/gerona/61.8.844. - DOI - PubMed
-
- McBean AM, Yu X. The underuse of screening services among elderly women with diabetes. Diabetes Care. 2007;30:1466–72. http://dx.doi.org/10.2337/dc06-2233. - DOI - PubMed
-
- Jaen CR, Stange KC, Nutting PA. Competing demands of primary care: a model for the delivery of clinical preventive services. J Fam Pract. 1994;38:166–71. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials