

The Role of Desmopressin in the Management of Severe, Hypovolemic Hyponatremia: A Single-Center, Comparative Analysis
- PMID: 29593879
- PMCID: PMC5865454
- DOI: 10.1177/2054358118761051
The Role of Desmopressin in the Management of Severe, Hypovolemic Hyponatremia: A Single-Center, Comparative Analysis
Abstract
Background: The role of desmopressin (DDAVP) to prevent or treat rapid serum sodium concentration ([Na]s) correction during hyponatremia management remains unclear.
Objective: To assess DDAVP use during the first 48 hours of severe, hypovolemic hyponatremia management. The primary study hypothesis was that the use of DDAVP would slow the rate of [Na]s correction compared with those not receiving DDAVP.
Design: A retrospective, observational, comparison study.
Setting: A single, Canadian, tertiary center.
Patients: All admitted patients referred to the nephrology service for severe, hypovolemic hyponatremia ([Na]s < 125 mmol/L) over a 12-month period from November 2015.
Measurements: The primary outcomes measure was the [Na]s after medical management for 48 hours. The length of hospital stay was also measured.
Methods: Patients were grouped based on whether they received DDAVP during the first 48 hours of treatment, and [Na]s correction was compared between groups using linear regression. An exploratory, multivariable, linear regression model was used to adjust for diabetes status, active malignancy, intensive care unit (ICU) admission, and hypertonic saline administration.
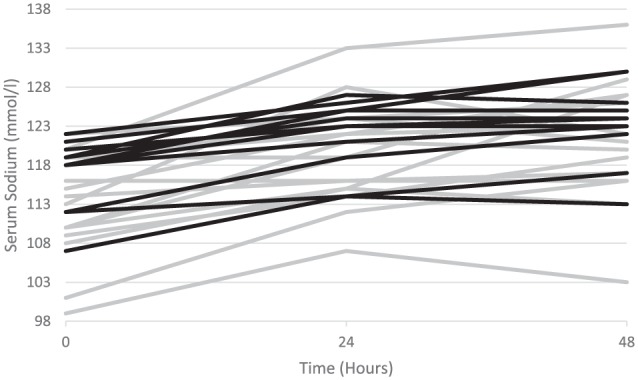
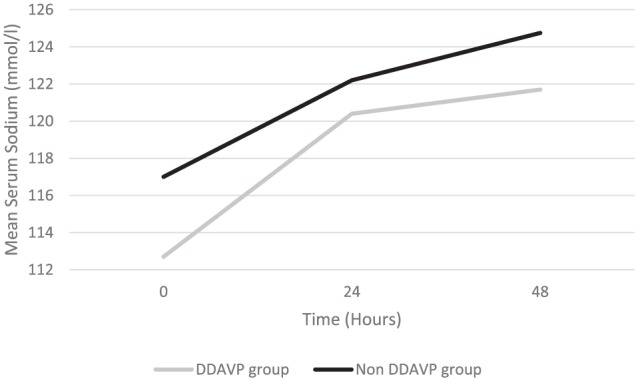
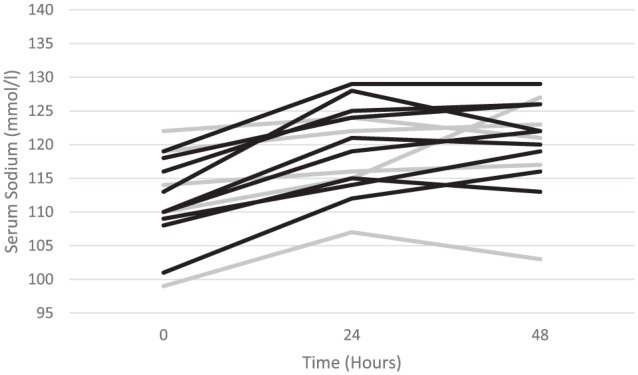
Results: Twenty-eight patients were identified, with baseline mean [Na]s of 112.7 ± 6.6 mmol/L versus 117 ± 4.3mmol/L (P = .06) in those receiving (n = 16) and not receiving DDAVP (n = 12), respectively. The DDAVP group had a more rapid [Na]s correction on the first day compared with those not receiving DDAVP, 7.7 ± 3.8 mmol/L/d versus 5.1 ± 2.0 mmol/L/d (P = .04). On the second day, there was a similar rate of [Na]s correction between groups: 1.3 ± 4.3 mmol/L/d versus 2.6 ± 3.2 mmol/L/d (P = .39), respectively. Overall, there was no difference in [Na]s correction after 48 hours between those who received DDAVP and those who did not: 121.7 ± 7.5 mmol/L versus 124.8 ± 5.7 mmol/L (P = .24). Patients who had experienced an overcorrection were successfully treated with DDAVP (n = 5), so that no patient had an ongoing overcorrection by 48 hours.
Limitations: The limited sample size and lack of randomization preclude definitive conclusion on the additional benefit of DDAVP to standard care.
Conclusion: DDAVP appears to be safe and effective in the management of severe, hypovolemic hyponatremia, associated with similar [Na]s correction to those who did not receive DDAVP after 48 hours, despite an initial more rapid correction. A randomized trial should examine what benefit DDAVP confers in addition to standard care in the management of severe, hypovolemic hyponatremia.
Contexte: Dans le contexte du traitement de l’hyponatrémie, le rôle de la desmopressine (DDAVP) pour prévenir et contrer la correction rapide de la concentration de sodium sérique ([Na] s) demeure nébuleux.
Objectif de l’étude: Notre objectif était d’étudier l’effet de l’administration de DDAVP au cours des 48 premières heures du traitement de l’hyponatrémie hypovolémique grave. L’hypothèse principale de l’étude était que l’administration de DDAVP ralentit le rythme de correction de la [Na] s chez les patients traités en comparaison des parents non traités.
Cadre et type d’étude: Il s’agit d’une étude comparative observationnelle, menée de façon rétrospective dans un centre de soins tertiaires canadien.
Patients: Ont été inclus tous les patients admis et ayant été dirigés vers l’unité de néphrologie en raison d’une hyponatrémie hypovolémique grave ([Na] s inférieure à 125 mmol/l) sur une période de douze mois à partir de novembre 2015.
Mesures: La [Na] s après les 48 premières heures de traitement constituait la mesure principale. On a également noté la durée de l’hospitalisation des patients.
Méthodologie: Les patients ont été regroupés selon qu’ils avaient reçu ou non de la DDAVP dans les 48 premières heures de traitement, et la comparaison de la correction de la [Na] s entre les groupes a été analysée par régression linéaire. Un modèle de régression linéaire multivariée et exploratoire a été utilisé pour ajuster les résultats en tenant compte de la présence de diabète, d’une affection maligne active, d’une admission à l’unité des soins intensifs et d’une administration de solution saline hypertonique.
Résultats: Un total de 28 patients a été retenu pour l’étude. La [Na] s initiale moyenne était de 112,7 ± 6,6 mmol/l pour les patients ayant reçu de la DDAVP (n = 16) contre 117 ± 4,3 mmol/l pour les douze patients du groupe non traité (P = 0,06). Dans le groupe traité, la correction de la [Na] s a été plus rapide au cours de la première journée comparativement à celle mesurée chez les patients non traités (7,7 ± 3,8 mmol/l/jour contre 5,1 ± 2,0 mmol/l/jour; P = 0,04). Le taux de correction de la [Na] s s’est avéré similaire dans les deux groupes au cours de la deuxième journée de suivi, avec des valeurs de 1,3 ± 4,3 mmol/l/jour pour le groupe ayant reçu de la DDAVP, et de 2,6 ± 3,2 mmol/l/jour pour le groupe non traité. Dans l’ensemble, aucune différence de correction de la [Na] s n’a été observée entre les deux groupes après 48 heures de suivi. Les valeurs se situaient alors à 121,7 ± 7,5 mmol/l pour les patients ayant reçu de la DDAVP et à 124,8 ± 5,7 mmol/l pour les patients non traités (P = 0,24). Cinq patients ont expérimenté une surcorrection et ont dû être traités à la DDAVP; le traitement a bien fonctionné, de sorte qu’aucun patient ne présentait de surcorrection après 48 heures.
Limites de l’étude: La taille restreinte de l’échantillon et l’absence de répartition aléatoire des cas nous empêchent de tirer une conclusion définitive quant à l’avantage supplémentaire apporté par l’ajout de la DDAVP aux procédures de soins courantes.
Conclusion: La DDAVP semble efficace et sécuritaire pour traiter l’hyponatrémie hypovolémique grave. Elle est associée à une correction similaire à celle mesurée après 48 heures chez les patients non traités, quoiqu’elle entraîne une correction initiale de la [Na] s plus rapide. Nous sommes d’avis qu’un essai clinique à répartition aléatoire devrait être mené pour étudier les bienfaits offerts par l’ajout de la DDAVP aux procédures de soins courantes contre l’hyponatrémie hypovolémique grave.
Keywords: DDAVP; antidiuretic hormone; desmopressin; hyponatremia; overcorrection.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Use of desmopressin acetate in severe hyponatremia in the intensive care unit.Clin J Am Soc Nephrol. 2014 Feb;9(2):229-37. doi: 10.2215/CJN.00950113. Epub 2013 Nov 21. Clin J Am Soc Nephrol. 2014. PMID: 24262506 Free PMC article.
-
Evaluation of Desmopressin in Critically Ill Patients with Hyponatremia Requiring 3% Hypertonic Saline.Am J Med Sci. 2021 Jun;361(6):711-717. doi: 10.1016/j.amjms.2021.03.012. Epub 2021 Apr 2. Am J Med Sci. 2021. PMID: 33812910
-
Outcomes in Severe Hyponatremia Treated With and Without Desmopressin.Am J Med. 2018 Mar;131(3):317.e1-317.e10. doi: 10.1016/j.amjmed.2017.09.048. Epub 2017 Oct 20. Am J Med. 2018. PMID: 29061503
-
The treatment of hyponatremia.Semin Nephrol. 2009 May;29(3):282-99. doi: 10.1016/j.semnephrol.2009.03.002. Semin Nephrol. 2009. PMID: 19523575 Review.
-
Management of severe hyponatremia: infusion of hypertonic saline and desmopressin or infusion of vasopressin inhibitors?Am J Med Sci. 2014 Nov;348(5):432-9. doi: 10.1097/MAJ.0000000000000331. Am J Med Sci. 2014. PMID: 25247759 Free PMC article. Review.
Cited by
-
Korean Society of Nephrology 2022 Recommendations on Controversial Issues in Diagnosis and Management of Hyponatremia.Electrolyte Blood Press. 2022 Jun;20(1):21-38. doi: 10.5049/EBP.2022.20.1.21. Epub 2022 Jun 30. Electrolyte Blood Press. 2022. PMID: 36451712 Free PMC article. Review.
-
Criteria for Hyponatremic Overcorrection: Systematic Review and Cohort Study of Emergently Ill Patients.J Gen Intern Med. 2020 Jan;35(1):315-321. doi: 10.1007/s11606-019-05286-y. Epub 2019 Aug 26. J Gen Intern Med. 2020. PMID: 31452039 Free PMC article.
-
The Effect of the Dose of Isotonic Saline on the Correction of Serum Sodium in the Treatment of Hypovolemic Hyponatremia.J Clin Med. 2020 Nov 5;9(11):3567. doi: 10.3390/jcm9113567. J Clin Med. 2020. PMID: 33167557 Free PMC article.
-
Korean Society of Nephrology 2022 recommendations on controversial issues in diagnosis and management of hyponatremia.Korean J Intern Med. 2022 Nov;37(6):1120-1137. doi: 10.3904/kjim.2022.174. Epub 2022 Oct 17. Korean J Intern Med. 2022. PMID: 36245341 Free PMC article. Review.
-
Safety and efficacy of proactive versus reactive administration of desmopressin in severe symptomatic hyponatremia: a randomized controlled trial.Sci Rep. 2024 Mar 29;14(1):7487. doi: 10.1038/s41598-024-57657-z. Sci Rep. 2024. PMID: 38553491 Free PMC article. Clinical Trial.
References
-
- Holland-Bill L, Christiansen CF, Heide-Jørgensen U, et al. Hyponatremia and mortality risk: a Danish cohort study of 279 508 acutely hospitalized patients. Eur J Endocrinol. 2015;173(1):71-81. - PubMed
-
- Whelan B, Bennett K, O’Riordan D, Silke B. Serum sodium as a risk factor for in-hospital mortality in acute unselected general medical patients. QJM. 2009;102:175-182. - PubMed
-
- Wald R, Jaber BL, Price LL, Upadhyay A, Madias NE. Impact of hospital-associated hyponatremia on selected outcomes. Arch Intern Med. 2010;170:294-302. - PubMed
-
- Spasovski G, Vanholder R, Allolio B, et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Nephrol Dial Transplant. 2014;29(suppl 2):i1-i39. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
