

Feasibility and Safety of Bariatric Surgery in High-Risk Patients: A Single-Center Experience
- PMID: 29593899
- PMCID: PMC5821962
- DOI: 10.1155/2018/7498258
Feasibility and Safety of Bariatric Surgery in High-Risk Patients: A Single-Center Experience
Abstract
Introduction: Despite the feasibility and safety of bariatric procedures nowadays, high-risk patients with vast obesity and severe comorbidities demonstrate relatively high perioperative morbidity and mortality rates and, therefore, form a distinguished challenge for the bariatric surgeons.
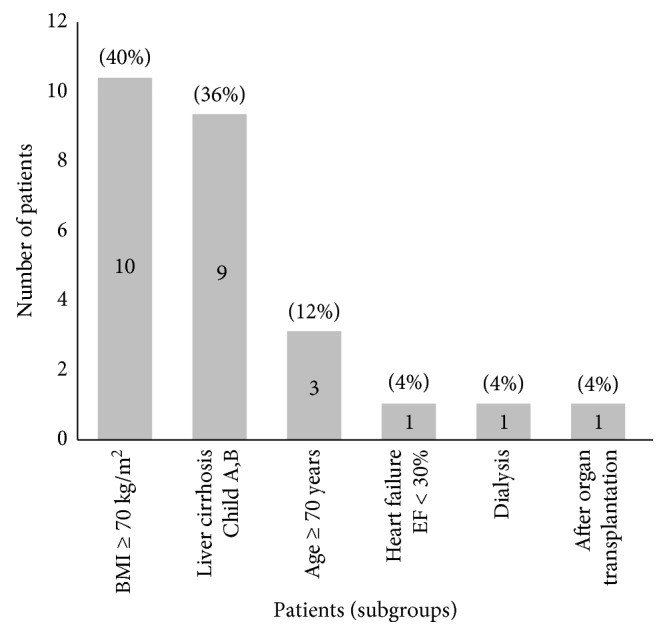
Methods: We retrospectively analyzed high-risk patients, who underwent bariatric surgery in University Hospital Leipzig between May 2012 and December 2016. High-risk patients were defined when (Bergeat et al., 2016) at least one of the following risk factors was met: age ≥ 70 years, body mass index (BMI) > 70 kg/m2, liver cirrhosis, end-organ failure, or immunosuppression by status after organ transplantation along with (Birkmeyer et al., 2010) at least two comorbidities associated with obesity. Our analysis included early postoperative complications.
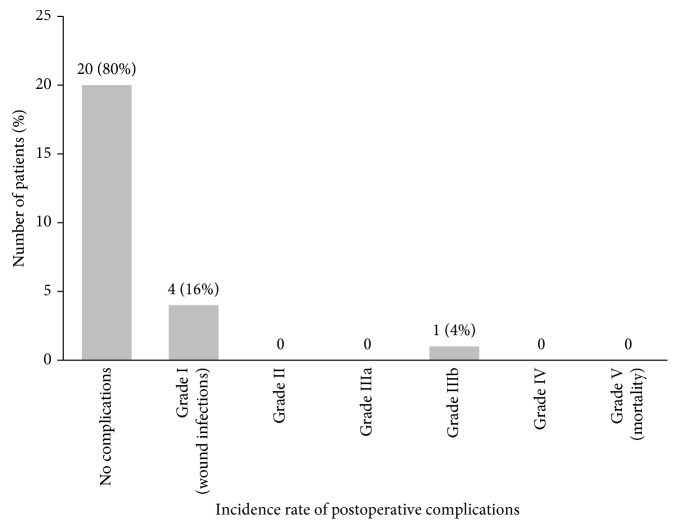
Results: A total of 25 high-risk obese patients were identified. All patients had a standardized postoperative management with a mean length of hospital stay of 4 ± 1.4 days. One patient required an operative revision due to a stapler line leak after sleeve gastrectomy. No other major postoperative complications occurred.
Conclusion: Bariatric surgery for severe high-risk patients can be performed safely in high-volume centers following standardized procedures.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
