

Angioplasty is an Effective Treatment for Vasospasm Following Pituitary Apoplexy and Tumor Resection
- PMID: 29593947
- PMCID: PMC5871324
- DOI: 10.7759/cureus.2117
Angioplasty is an Effective Treatment for Vasospasm Following Pituitary Apoplexy and Tumor Resection
Abstract
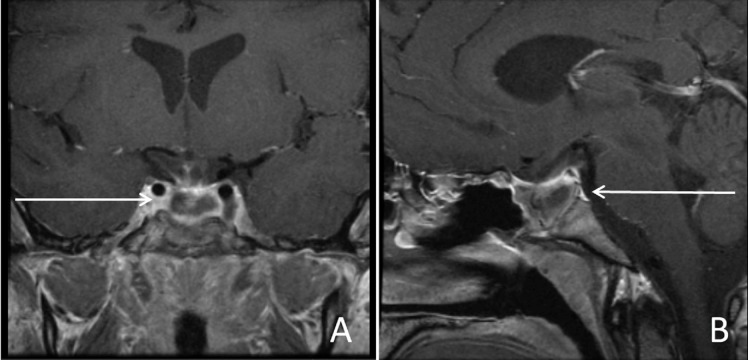
Pituitary apoplexy is a clinical syndrome characterized by acute headache, visual changes, and decreased consciousness occurring in association with hemorrhage or infarct of an existing pituitary adenoma. Surgical management involves tumor resection and decompression of surrounding structures including the optic apparatus. Vasospasm is a rare but potentially devastating complication of pituitary apoplexy. We present a case of pituitary apoplexy in a 28-year-old male treated with emergent endoscopic transsphenoidal resection. On postoperative day seven, following surgical resection, the patient developed neurologic deficits and motor weakness, and severe vasospasm was diagnosed. This is a novel case of intra-arterial verapamil and angioplasty used to treat vasospasm following surgical decompression for pituitary apoplexy. The patient experienced complete recovery of motor deficits following treatment. The authors propose angioplasty as an effective treatment for postoperative vasospasm following transphenoidal surgery for pituitary apoplexy in the presence of focal vessel stenosis.
Keywords: angioplasty; endovascular; pituitary apoplexy; vasospasm; verapamil.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





Similar articles
-
Cerebral vasospasm as a consequence of pituitary apoplexy: illustrative case.J Neurosurg Case Lessons. 2023 Feb 13;5(7):CASE22349. doi: 10.3171/CASE22349. Print 2023 Feb 13. J Neurosurg Case Lessons. 2023. PMID: 36794733 Free PMC article.
-
Emergency endoscopic surgery for pituitary apoplexy presenting as cerebral infarction in a limited resources condition: A case report.Int J Surg Case Rep. 2021 Jun;83:106015. doi: 10.1016/j.ijscr.2021.106015. Epub 2021 May 26. Int J Surg Case Rep. 2021. PMID: 34118525 Free PMC article.
-
Endoscopic Endonasal Transsphenoidal Resection for Pituitary Apoplexy during the Third Trimester of Pregnancy.Surg Res Pract. 2014;2014:397131. doi: 10.1155/2014/397131. Epub 2014 Jan 2. Surg Res Pract. 2014. PMID: 25374951 Free PMC article.
-
Surgical treatment of pituitary apoplexy in association with hemispheric infarction.J Clin Neurosci. 2015 Oct;22(10):1550-4. doi: 10.1016/j.jocn.2015.03.049. Epub 2015 Jul 23. J Clin Neurosci. 2015. PMID: 26213287 Review.
-
Postoperative Cerebral Vasospasm Following Transsphenoidal Pituitary Adenoma Surgery.World Neurosurg. 2016 Aug;92:7-14. doi: 10.1016/j.wneu.2016.04.099. Epub 2016 May 4. World Neurosurg. 2016. PMID: 27155378 Review.
Cited by
-
Symptomatic Cerebral Vasospasm After Transsphenoidal Tumor Resection: Two Case Reports and Systematic Literature Review.Cureus. 2020 May 17;12(5):e8171. doi: 10.7759/cureus.8171. Cureus. 2020. PMID: 32566415 Free PMC article. Review.
References
-
- Pituitary apoplexy: evaluation, management, and prognosis. Murad-Kejbou S, Eggenberger E. Curr Opin Ophthalmol. 2009;20:456–461. - PubMed
-
- Management and outcomes of pituitary apoplexy. Singh TD, Valizadeh N, Meyer FB, et al. J Neurosurg. 2015;122:1450–1457. - PubMed
-
- Cerebral infarction caused by pituitary apoplexy: case report and review of literature. Zhang C, Feng F, Zhu Y, et al. Turk Neurosurg. 2014;24:782–787. - PubMed
-
- Cerebral ischaemia in pituitary apoplexy. Ahmed SK, Semple PL. Acta Neurochir. 2008;150:1193–1196. - PubMed
-
- Cerebral ischemia in pituitary disorders- more common than previously thought: two case reports and literature review. Chong MY, Quak SM, Chong CT. Pituitary. 2014;17:171–179. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources