

Late-onset endometrial ablation failure
- PMID: 29593995
- PMCID: PMC5842972
- DOI: 10.1016/j.crwh.2017.07.001
Late-onset endometrial ablation failure
Abstract
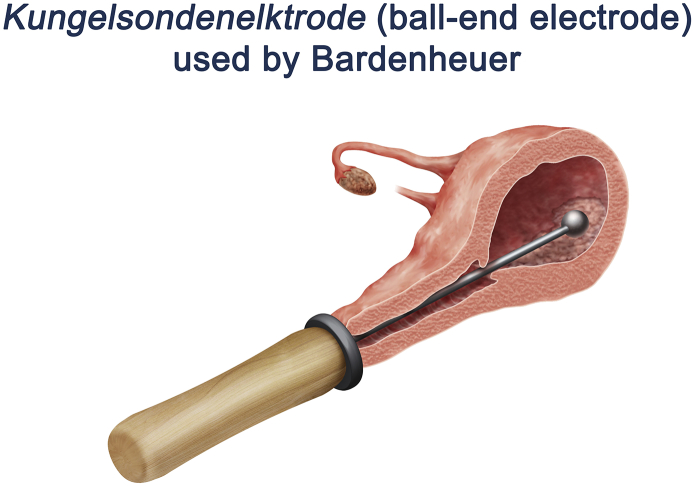
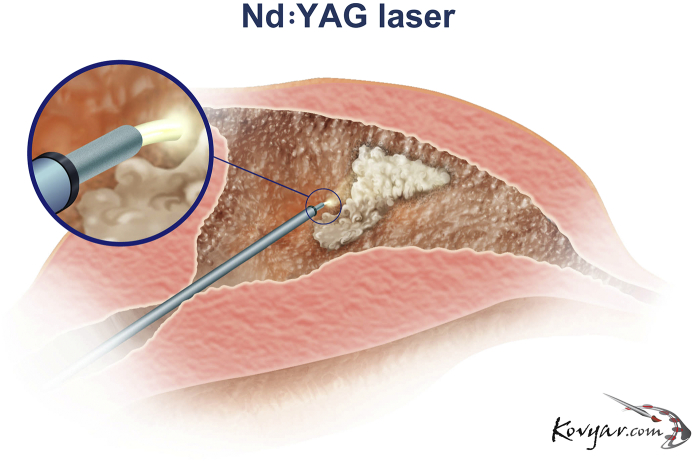
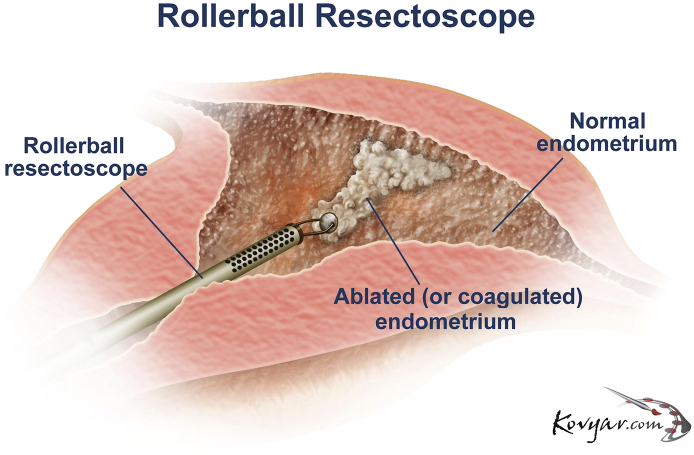
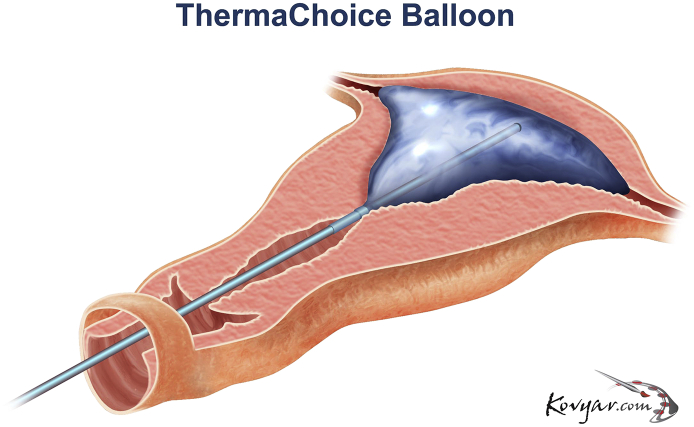
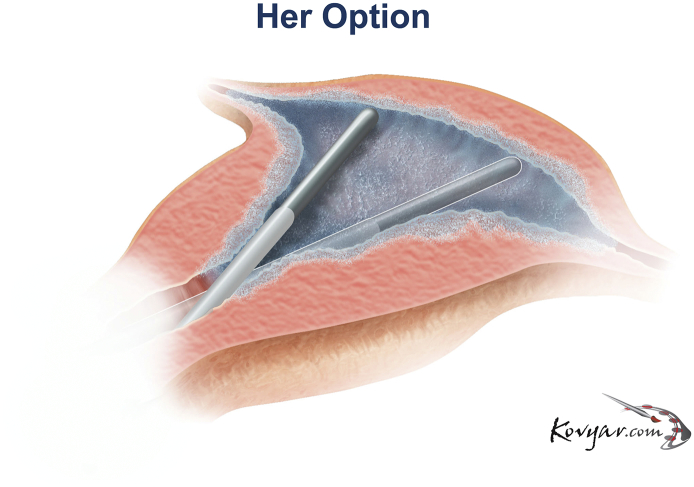
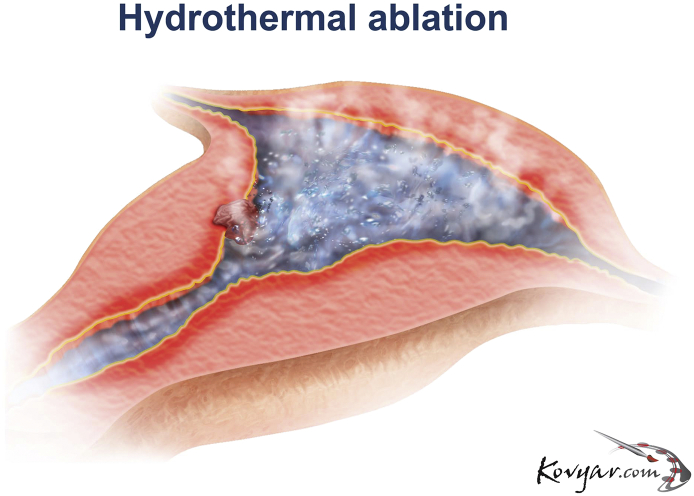
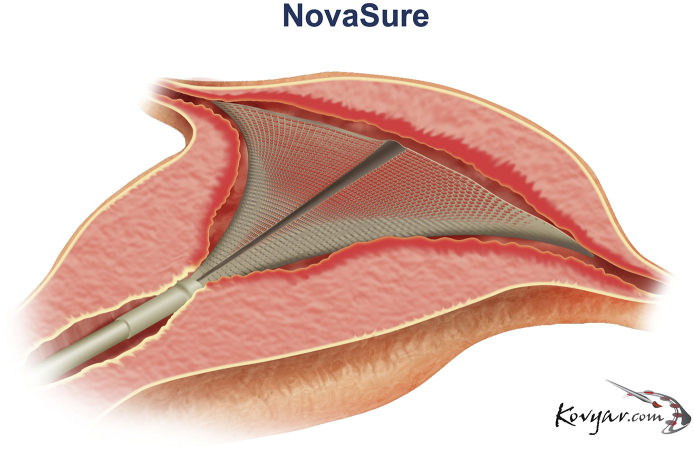
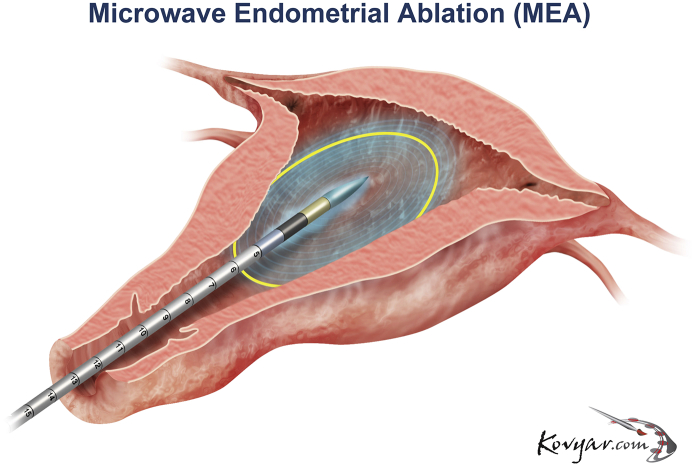
Endometrial ablation, first reported in the 19th century, has gained wide acceptance in the gynecologic community as an important tool for the management of abnormal uterine bleeding when medical management has been unsuccessful or contraindicated. The introduction of global endometrial ablation (GEA) devices beginning in 1997 has provided unsurpassed safety addressing many of the concerns associated with their resectoscopic predecessors. As of this writing the GEA market has surpassed a half-million devices in the United States per annum and has an expected compound annual growth rate (CAGR) projected to be 5.5% from 2016 to 2024. While the short term safety and efficacy of these devices has been reported in numerous clinical trials we only recently are becoming aware of the high incidence of late-onset endometrial ablation failures (LOEAFs) associated with these procedures. Currently, about a quarter of women who undergo a GEA procedure will eventually require a hysterectomy while an unknown number have less than satisfactory results. In order to reduce these suboptimal outcomes physicians must better understand the etiology and risk factors that predispose a patient toward the development of LOEAF as well as current knowledge of patient and procedure selection for EA as well as treatment options for these delayed complications.
Figures


Similar articles
-
Endometrial ablation in the management of abnormal uterine bleeding.J Obstet Gynaecol Can. 2015 Apr;37(4):362-79. doi: 10.1016/s1701-2163(15)30288-7. J Obstet Gynaecol Can. 2015. PMID: 26001691
-
Post-Ablation Endometrial Carcinoma (PAEC) Following Radiofrequency Endometrial Ablation: A Case Report and Its Implications for Management of Endometrial Ablation Failures.Surg Technol Int. 2016 Oct 26;29:161-166. Surg Technol Int. 2016. PMID: 27608750
-
Endometrial ablation.Best Pract Res Clin Obstet Gynaecol. 2018 Jan;46:120-139. doi: 10.1016/j.bpobgyn.2017.10.003. Epub 2017 Oct 20. Best Pract Res Clin Obstet Gynaecol. 2018. PMID: 29128205 Review.
-
Economic Evaluation of Global Endometrial Ablation Versus Inpatient and Outpatient Hysterectomy for Treatment of Abnormal Uterine Bleeding: US Commercial and Medicaid Payer Perspectives.Popul Health Manag. 2018 Mar;21(S1):S1-S12. doi: 10.1089/pop.2017.0172. Popul Health Manag. 2018. PMID: 29570003
-
Endometrial ablation or resection versus levonorgestrel intra-uterine system for the treatment of women with heavy menstrual bleeding and a normal uterine cavity: a systematic review with meta-analysis.Hum Reprod Update. 2020 Feb 28;26(2):302-311. doi: 10.1093/humupd/dmz051. Hum Reprod Update. 2020. PMID: 31990359
Cited by
-
Endometrial Cryoablation for the Treatment of Heavy Menstrual Bleeding: 36-Month Outcomes from the CLARITY Study.Int J Womens Health. 2022 Aug 10;14:1083-1092. doi: 10.2147/IJWH.S371044. eCollection 2022. Int J Womens Health. 2022. PMID: 35983177 Free PMC article.
-
Modified Thermal Balloon Endometrial Ablation for Treatment of Heavy Menstrual Bleeding.Gynecol Minim Invasive Ther. 2022 May 4;11(2):100-104. doi: 10.4103/GMIT.GMIT_147_20. eCollection 2022 Apr-Jun. Gynecol Minim Invasive Ther. 2022. PMID: 35746908 Free PMC article.
-
Pitfalls and Strategies for Measuring Menopausal Stage in Eating Disorder Studies of Women in Midlife.Int J Eat Disord. 2025 Jun;58(6):1008-1017. doi: 10.1002/eat.24414. Epub 2025 Mar 14. Int J Eat Disord. 2025. PMID: 40084592 Free PMC article.
-
Mechanisms of Regeneration and Fibrosis in the Endometrium.Annu Rev Cell Dev Biol. 2023 Oct 16;39:197-221. doi: 10.1146/annurev-cellbio-011723-021442. Annu Rev Cell Dev Biol. 2023. PMID: 37843929 Free PMC article. Review.
References
-
- Leape LL, Bernstein SJ, Bohon CJ, Dickerson VM, Ling FW, Shiffman RN, Kanouse DE. Hysterectomy: Clinical Recommendations and Indications for Use. Southern California Health Policy Research Consortium. RAND.
-
- Munro M.G. ACOG practice bulletin: endometrial ablation. Obstet. Gynecol. 2007;109:1233–1247. - PubMed
-
- Longinotti M.K., Jacobson G.F., Hung Y.Y., Learman L.A. Probability of hysterectomy after endometrial ablation. Obstet. Gynecol. 2008;112:1214–1220. - PubMed
-
- Sharp J.T. Endometrial ablation: postoperative complications. Am. J. Obstet. Gynecol. 2012;207:242–247. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
