

Multivariable risk-based patient selection for prostate biopsy in a primary health care setting: referral rate and biopsy results from a urology outpatient clinic
- PMID: 29594017
- PMCID: PMC5861274
- DOI: 10.21037/tau.2017.12.11
Multivariable risk-based patient selection for prostate biopsy in a primary health care setting: referral rate and biopsy results from a urology outpatient clinic
Abstract
Background: According to their guidelines, Dutch general practitioners (GPs) refer men with prostate-specific antigen (PSA) level ≥3.0 ng/mL to the urologist for risk-based patient selection for prostate biopsy using the Rotterdam Prostate Cancer Risk Calculator (RPCRC). Use of the RPCRC in primary care could optimize the diagnostic pathway even further by reducing unnecessary referrals. To investigate this, we calculated the risk and assessed the rate of men referred to the urologist with PSA level ≥3.0 ng/mL by implementing the RPCRC in a primary health care setting.
Methods: In January 2014, an exploratory study was initiated in collaboration with the primary health care facility of the GP laboratory in Rotterdam. GPs were given the possibility to refer men with a suspicion of prostate cancer (PCa) or a screening wish to this primary care facility (STAR-SHL) where further assessment was performed by specially trained personnel. Risk-based advice on referral to the urologist was given to the GP on the basis of the RPCRC results. If requested, advice on the treatment of lower urinary tract symptoms (LUTS) was provided. All men signed informed consent.
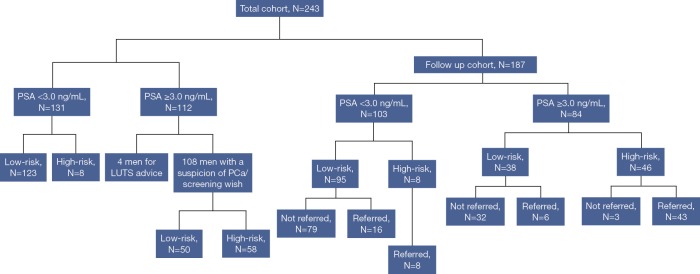
Results: Between January 2014 and September 2017, a total of 243 men, median age 64 [interquartile range (IQR), 57-70] years were referred for a consultation at the primary care facility. Of the 108 men with PSA level ≥3.0 ng/mL and a referral related to PCa, GPs were advised to refer 58 men to the urologist (54%). Of the men with available follow-up (FU) data [n=187, median FU, 16 (IQR, 9-25) months] 54 men were considered high-risk (i.e., had an elevated risk of PCa as calculated by the RPCRC). Of these men, 51 (94%) were actually referred to secondary care by their GP, and so far 38 men underwent biopsy. PCa was detected in 30 men [47% had Gleason score (GS) ≥3+4 PCa], translating to an overall positive predictive value (PPV) of 79%. Within the available FU time, 2 out of 38 (5%) men with PSA level ≥3.0 ng/mL which were considered low-risk have been diagnosed with GS 3+3 PCa.
Conclusions: Risk-stratification with the RPCRC in a primary health care setting could prevent almost half of referrals of men with PSA level ≥3.0 ng/mL to the urologist. In more than three-quarters of men referred for prostate biopsy, the suspicion of PCa was confirmed and almost half of men had clinically significant PCa (GS ≥3+4 PCa). These data show a huge potential for multivariable risk-stratification in primary care.
Keywords: Primary care; prostate cancer; prostate volume; prostate-specific antigen (PSA); risk-stratification.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Prostate cancer risk assessment by the primary care physician and urologist: transabdominal- versus transrectal ultrasound prostate volume-based use of the Rotterdam Prostate Cancer Risk Calculator.Transl Androl Urol. 2023 Feb 28;12(2):241-248. doi: 10.21037/tau-22-640. Epub 2023 Feb 1. Transl Androl Urol. 2023. PMID: 36915892 Free PMC article.
-
Shifting risk-stratified early prostate cancer detection to a primary healthcare setting.BJU Int. 2023 May;131(5):596-601. doi: 10.1111/bju.15933. Epub 2022 Dec 19. BJU Int. 2023. PMID: 36408660
-
Risk-based Patient Selection for Magnetic Resonance Imaging-targeted Prostate Biopsy after Negative Transrectal Ultrasound-guided Random Biopsy Avoids Unnecessary Magnetic Resonance Imaging Scans.Eur Urol. 2016 Jun;69(6):1129-34. doi: 10.1016/j.eururo.2015.11.018. Epub 2015 Dec 2. Eur Urol. 2016. PMID: 26651990
-
Multiparametric MRI in detection and staging of prostate cancer.Dan Med J. 2017 Feb;64(2):B5327. Dan Med J. 2017. PMID: 28157066 Review.
-
Active Surveillance Use Among a Low-risk Prostate Cancer Population in a Large US Payer System: 17-Gene Genomic Prostate Score Versus Other Risk Stratification Methods.Rev Urol. 2017;19(4):203-212. doi: 10.3909/riu0786. Rev Urol. 2017. PMID: 29472824 Free PMC article. Review.
Cited by
-
Head and neck cancer risk calculator (HaNC-RC)-V.2. Adjustments and addition of symptoms and social history factors.Clin Otolaryngol. 2020 May;45(3):380-388. doi: 10.1111/coa.13511. Epub 2020 Feb 20. Clin Otolaryngol. 2020. PMID: 31985180 Free PMC article.
-
Predicting the risk of prostate cancer in asymptomatic men: a cohort study to develop and validate a novel algorithm.Br J Gen Pract. 2021 Apr 29;71(706):e364-e371. doi: 10.3399/bjgp20X714137. Print 2021 May. Br J Gen Pract. 2021. PMID: 33875417 Free PMC article.
-
Prostate cancer risk assessment by the primary care physician and urologist: transabdominal- versus transrectal ultrasound prostate volume-based use of the Rotterdam Prostate Cancer Risk Calculator.Transl Androl Urol. 2023 Feb 28;12(2):241-248. doi: 10.21037/tau-22-640. Epub 2023 Feb 1. Transl Androl Urol. 2023. PMID: 36915892 Free PMC article.
-
PSA testing in primary care: is it time to change our practice?BMC Prim Care. 2024 Dec 26;25(1):436. doi: 10.1186/s12875-024-02688-8. BMC Prim Care. 2024. PMID: 39725949 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous