

MRI in early prostate cancer detection: how to manage indeterminate or equivocal PI-RADS 3 lesions?
- PMID: 29594022
- PMCID: PMC5861283
- DOI: 10.21037/tau.2017.12.31
MRI in early prostate cancer detection: how to manage indeterminate or equivocal PI-RADS 3 lesions?
Abstract
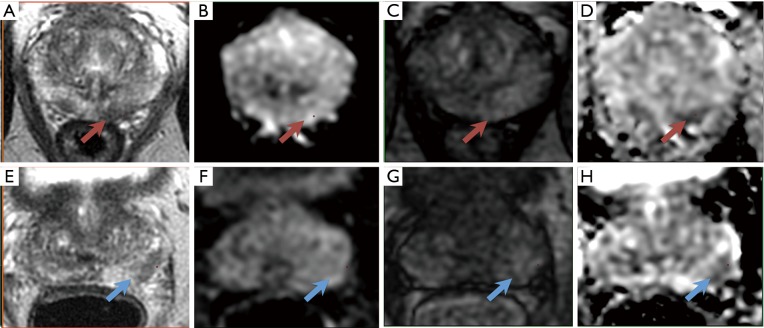
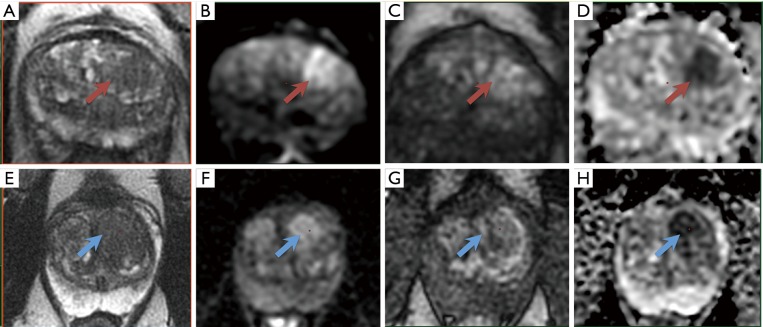
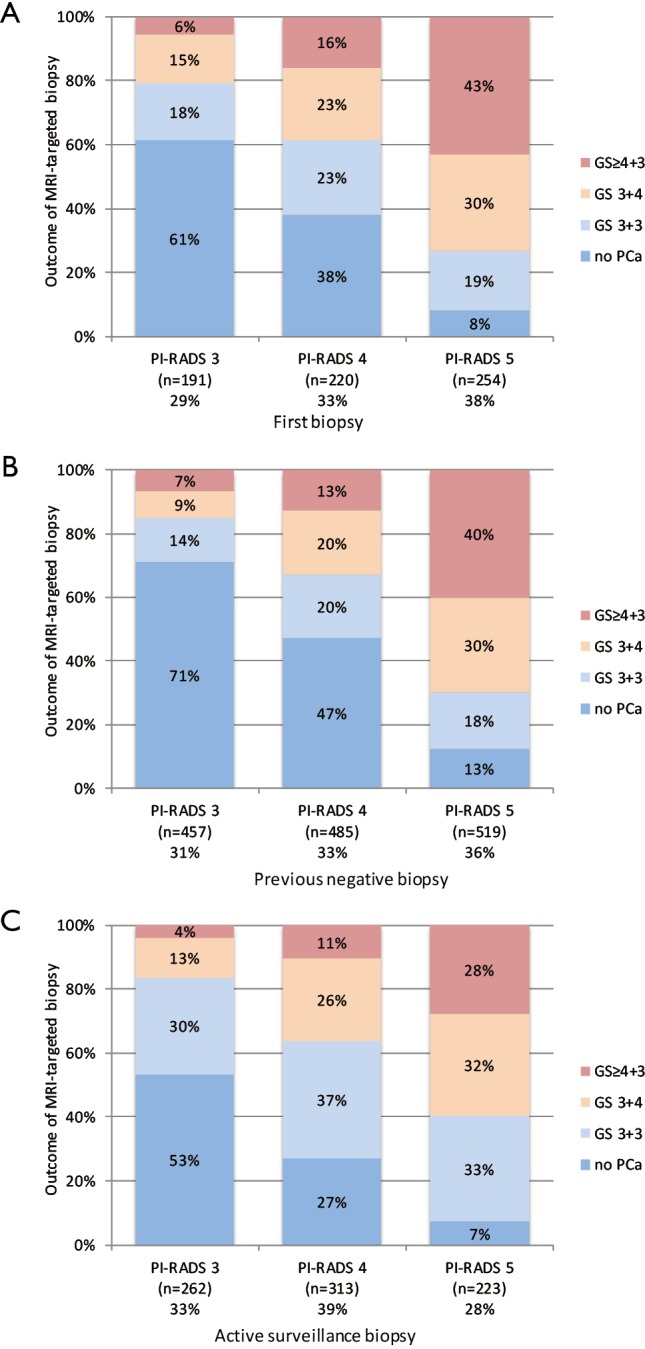
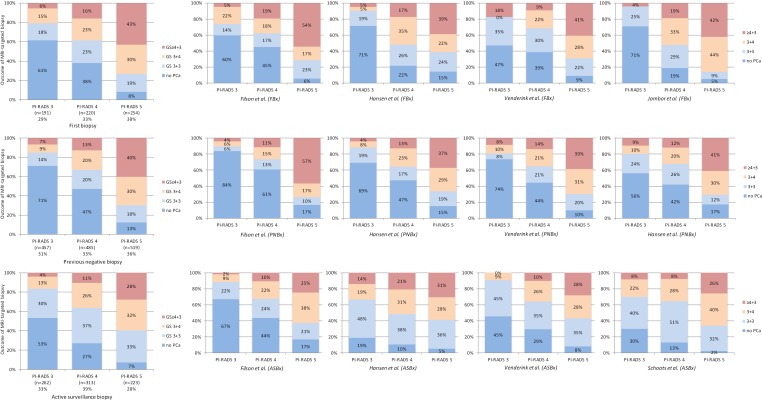
This review focuses on indeterminate lesions on prostate magnetic resonance imaging (MRI), assigned as PI-RADS category 3. The prevalence of PI-RADS 3 index lesion in the diagnostic work-up is significant, varying between one in three (32%) to one in five (22%) men, depending on patient cohort of first biopsies, previously negative biopsies, and active surveillance biopsies. A management strategy must be developed for this group of men with an indeterminate suspicion of having clinically significant prostate cancer (csPCa). Currently available data show that the actual prevalence of csPCa after targeted biopsy in PI-RADS 3 lesions vary between patients groups from one in five (21%) to one in six (16%), depending on previous biopsy status. Although this prevalence is lower in comparison to PI-RADS 4 and PI-RADS 5 lesions, still a considerable proportion of men harbor significant disease. Men with such a PI-RADS 3 lesion should therefore be adequately managed. In general, the clinical approach of using a threshold of PI-RADS ≥4 instead of PI-RADS ≥3 to select MRI for targeted biopsies is not supported by data from our explorative literature search using current definitions of csPCa. A possible adaptation to the threshold of PI-RADS ≥4 in combination with other clinical markers could be considered within an active surveillance protocol, where the balance between the individual risk of missing csPCa and the constant process of repeating prostate biopsies is crucial. In the future, improvements in MR imaging and interpretation, combined with molecular biomarkers and multivariate risk models will all be employed in prostate cancer detection and monitoring. These combinations will aid decision-making in challenging circumstances, such as unclear and diagnostic equivocal results for csPCa at early detection.
Keywords: MRI-guided targeted biopsy; PI-RADS; PI-RADS 3; PSA density; Prostate cancer; biopsy; equivocal; indeterminate; magnetic resonance imaging (MRI); risk stratification.
Conflict of interest statement
Conflicts of Interest: The author has no conflicts of interest to declare.
Figures
References
-
- Moldovan PC, Van den Broeck T, Sylvester R, et al. What Is the Negative Predictive Value of Multiparametric Magnetic Resonance Imaging in Excluding Prostate Cancer at Biopsy? A Systematic Review and Meta-analysis from the European Association of Urology Prostate Cancer Guidelines Panel. Eur Urol 2017;72:250-66. 10.1016/j.eururo.2017.02.026 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous