

Active surveillance for prostate cancer: a systematic review of contemporary worldwide practices
- PMID: 29594023
- PMCID: PMC5861285
- DOI: 10.21037/tau.2017.12.24
Active surveillance for prostate cancer: a systematic review of contemporary worldwide practices
Abstract
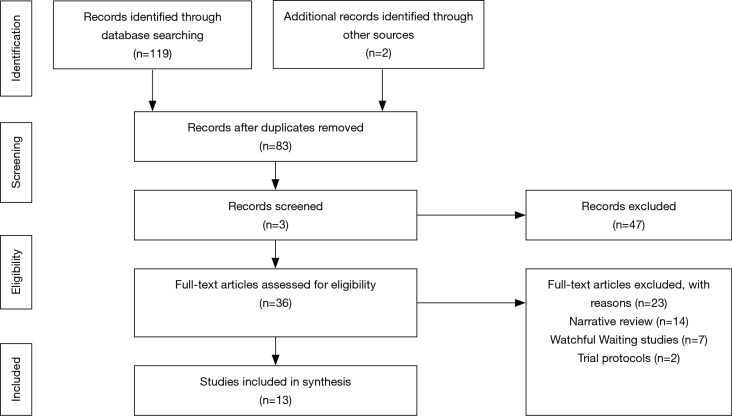
In the last decade, active surveillance (AS) has emerged as an acceptable choice for low-risk prostate cancer (PC), however there is discordance amongst large AS cohort studies with respect to entry and monitoring protocols. We systematically reviewed worldwide AS practices in studies reporting ≥5 years follow-up. We searched PubMed and Medline 2000-now and identified 13 AS cohorts. Three key areas were identified: (I) patient selection; (II) monitoring protocols; (III) triggers for intervention-(I) all studies defined clinically localised PC diagnosis as T2b disease or less and most agreed on prostate-specific antigen (PSA) threshold (<10 µg/L) and Gleason score threshold (3+3). Inconsistency was most notable regarding pathologic factors (e.g., number of positive cores); (II) all agreed on PSA surveillance as crucial for monitoring, and most agreed that confirmatory biopsy was required within 12 months of initiation. No consensus was reached on optimal timing of digital rectal examination (DRE), general health assessment or re-biopsy strategies thereafter; (III) there was no universal agreement for intervention triggers, although Gleason score, number or percentage of positive cancer cores, maximum cancer length (MCL) and PSA doubling time were used by several studies. Some also used imaging or re-biopsy. Despite consistent high progression-free/cancer-free survival and conversion-to-treatment rates, heterogeneity exists amongst these large AS cohorts. Combining existing evidence and gathering more long-term evidence [e.g., the Movember's Global AS database or additional information on use of magnetic resonance imaging (MRI)] is needed to derive a broadly supported guideline to reduce variation in clinical practice.
Keywords: Active surveillance (AS); cohort study; prostate cancer (PC).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Network NCI. Cancer incidence, males, ICD10 C61: Prostate, 2008-2010. National Cancer Intelligence Network (NCIN), UK Cancer Information Service (UKCIS). UKCIS. 2010.
-
- Dall’Era MA. The economics of active surveillance for prostate cancer. Curr Opin Urol 2013;23:278-82. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous