

The EMBRACE II study: The outcome and prospect of two decades of evolution within the GEC-ESTRO GYN working group and the EMBRACE studies
- PMID: 29594251
- PMCID: PMC5862686
- DOI: 10.1016/j.ctro.2018.01.001
The EMBRACE II study: The outcome and prospect of two decades of evolution within the GEC-ESTRO GYN working group and the EMBRACE studies
Abstract
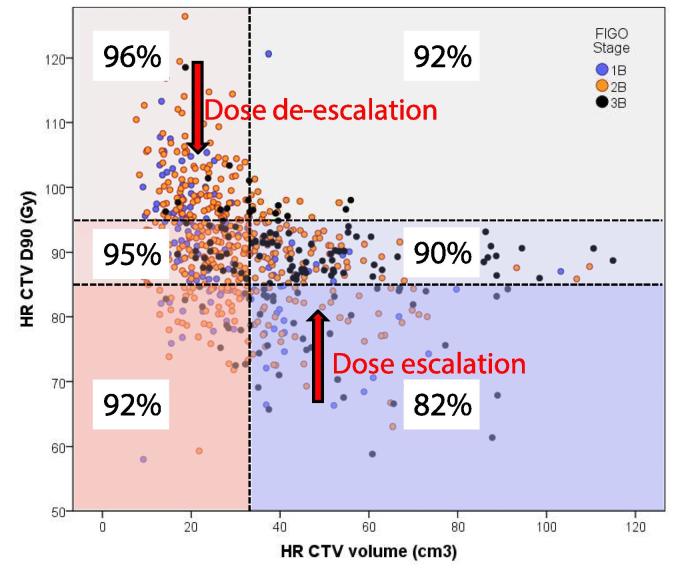
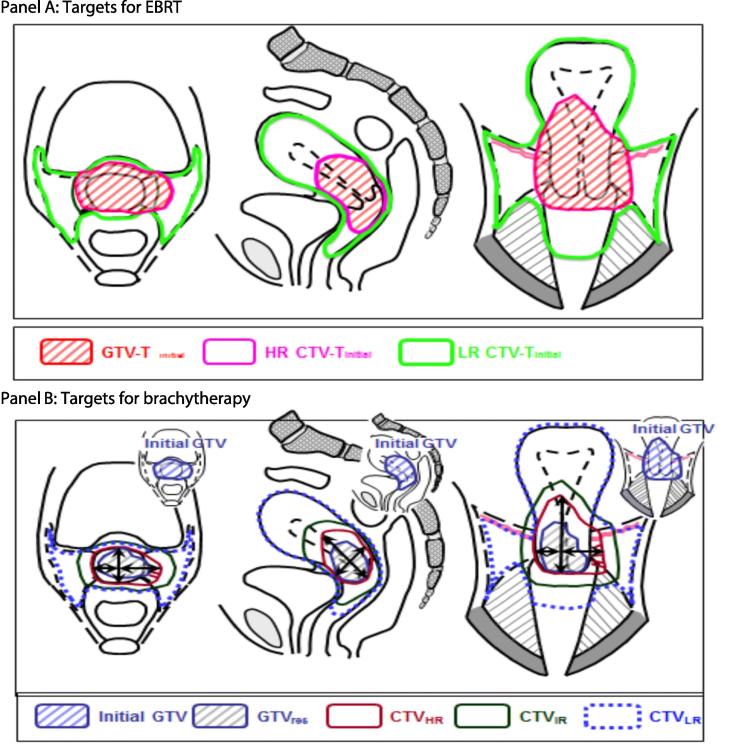
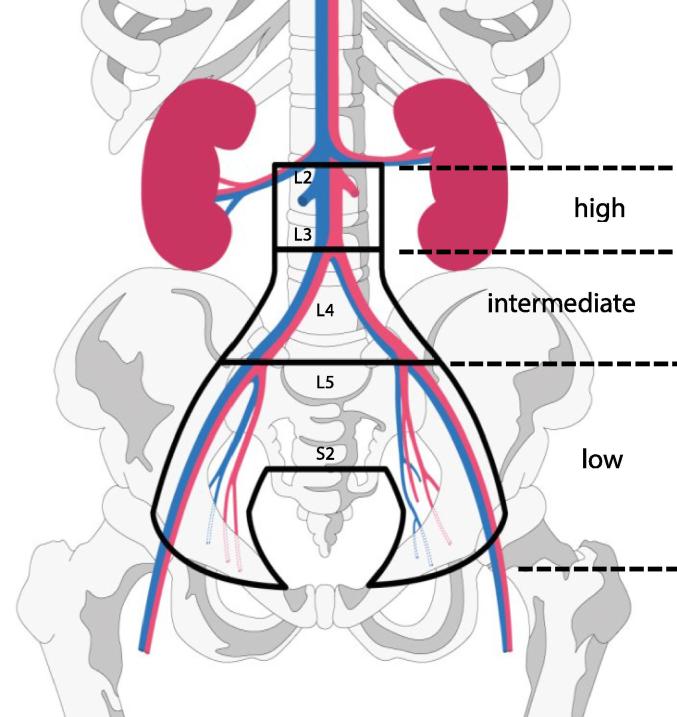
The publication of the GEC-ESTRO recommendations one decade ago was a significant step forward for reaching international consensus on adaptive target definition and dose reporting in image guided adaptive brachytherapy (IGABT) in locally advanced cervical cancer. Since then, IGABT has been spreading, particularly in Europe, North America and Asia, and the guidelines have proved their broad acceptance and applicability in clinical practice. However, a unified approach to volume contouring and reporting does not imply a unified administration of treatment, and currently both external beam radiotherapy (EBRT) and IGABT are delivered using a large variety of techniques and prescription/fractionation schedules. With IGABT, local control is excellent in limited and well-responding tumours. The major challenges are currently loco-regional control in advanced tumours, treatment-related morbidity, and distant metastatic disease. Emerging evidence from the RetroEMBRACE and EMBRACE I studies has demonstrated that clinical outcome is related to dose prescription and technique. The next logical step is to demonstrate excellent clinical outcome with the most advanced EBRT and brachytherapy techniques based on an evidence-based prospective dose and volume prescription protocol. The EMBRACE II study is an interventional and observational multicentre study which aims to benchmark a high level of local, nodal and systemic control while limiting morbidity, using state of the art treatment including an advanced target volume selection and contouring protocol for EBRT and brachytherapy, a multi-parametric brachytherapy dose prescription protocol (clinical validation of dose constraints), and use of advanced EBRT (IMRT and IGRT) and brachytherapy (IC/IS) techniques (clinical validation). The study also incorporates translational research including imaging and tissue biomarkers.
Keywords: Adaptive radiotherapy; Brachytherapy; Cervix cancer; Local control; MRI guided radiotherapy; Morbidity.
Figures

References
-
- Haie-Meder C., Pötter R., Van Limbergen E., Briot E., De Brabandere M., Dimopoulos J. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group☆ (I): concepts and terms in 3D image based 3D treatment planning in cervix cancer brachytherapy with emphasis on MRI assessment of GTV and CTV. Radiother Oncol. 2005;74:235–245. - PubMed
-
- Pötter R., Haie-Meder C., Van Limbergen E., Barillot I., De Brabandere M., Dimopoulos J. Recommendations from gynaecological (GYN) GEC ESTRO working group (II): concepts and terms in 3D image-based treatment planning in cervix cancer brachytherapy-3D dose volume parameters and aspects of 3D image-based anatomy, radiation physics, radiobiology. Radiother Oncol. 2006;78:67–77. - PubMed
-
- Hellebust T.P., Kirisits C., Berger D., Pérez-Calatayud J., De Brabandere M., De Leeuw A. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group: considerations and pitfalls in commissioning and applicator reconstruction in 3D image-based treatment planning of cervix cancer brachytherapy. Radiother Oncol. 2010;96:153–160. - PubMed
-
- Dimopoulos J.C.A., Petrow P., Tanderup K., Petric P., Berger D., Kirisits C. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (IV): Basic principles and parameters for MR imaging within the frame of image based adaptive cervix cancer brachytherapy. Radiother Oncol. 2012;103:113–122. - PMC - PubMed
-
- Tan L.T. Implementation of Image-guided Brachytherapy for Cervix Cancer in the UK: progress Update. Clin Oncol. 2011;23:681–684. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
