

One-Year Outcomes in Patients With Acute Respiratory Distress Syndrome Enrolled in a Randomized Clinical Trial of Helmet Versus Facemask Noninvasive Ventilation
- PMID: 29595563
- PMCID: PMC6005726
- DOI: 10.1097/CCM.0000000000003124
One-Year Outcomes in Patients With Acute Respiratory Distress Syndrome Enrolled in a Randomized Clinical Trial of Helmet Versus Facemask Noninvasive Ventilation
Abstract
Objectives: Many survivors of acute respiratory distress syndrome have poor long-term outcomes possibly due to supportive care practices during "invasive" mechanical ventilation. Helmet noninvasive ventilation in acute respiratory distress syndrome may reduce intubation rates; however, it is unknown if avoiding intubation with helmet noninvasive ventilation alters the consequences of surviving acute respiratory distress syndrome.
Design: Long-term follow-up data from a previously published randomized controlled trial.
Patients: Adults patients with acute respiratory distress syndrome enrolled in a previously published clinical trial.
Setting: Adult ICU.
Intervention: None.
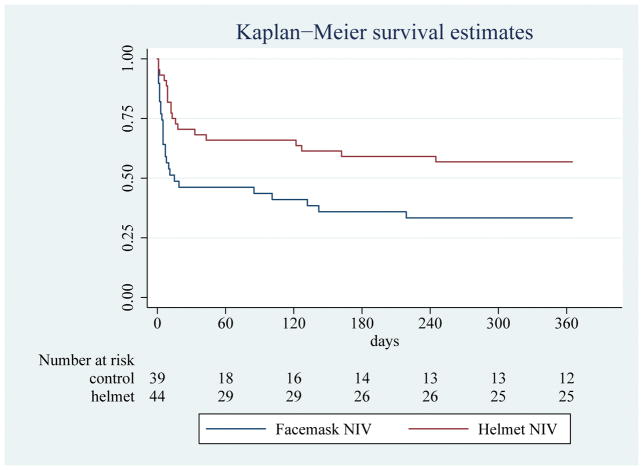
Measurements and main results: The primary outcome was functional independence at 1 year after hospital discharge defined as independence in activities of daily living and ambulation. At 1 year, patients were surveyed to assess for functional independence, survival, and number of institution-free days, defined as days alive spent living at home. The presence of ICU-acquired weakness and functional independence was also assessed by a blinded therapist on hospital discharge. On hospital discharge, there was a greater prevalence of ICU-acquired weakness (79.5% vs 38.6%; p = 0.0002) and less functional independence (15.4% vs 50%; p = 0.001) in the facemask group. One-year follow-up data were collected for 81 of 83 patients (97.6%). One-year mortality was higher in the facemask group (69.2% vs 43.2%; p = 0.017). At 1 year, patients in the helmet group were more likely to be functionally independent (40.9% vs 15.4%; p = 0.015) and had more institution-free days (median, 268.5 [0-354] vs 0 [0-323]; p = 0.017).
Conclusions: Poor functional recovery after invasive mechanical ventilation for acute respiratory distress syndrome is common. Helmet noninvasive ventilation may be the first intervention that mitigates the long-term complications that plague survivors of acute respiratory distress syndrome managed with noninvasive ventilation.
Conflict of interest statement
We declare that we have no relevant conflicts of interest.
Figures
Comment in
-
Is Helmet Noninvasive Ventilation a Protective Factor for Long-Term Outcome in Acute Respiratory Distress Syndrome?Crit Care Med. 2019 Feb;47(2):e164. doi: 10.1097/CCM.0000000000003458. Crit Care Med. 2019. PMID: 30653084 No abstract available.
References
-
- Herridge MS, Tansey CM, Matte A, et al. Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med. 2011;364:1293–304. - PubMed
-
- Nydahl P, Ruhl AP, Bartoszek G, et al. Early mobilization of mechanically ventilated patients: a 1-day point-prevalence study in Germany. Crit Care Med. 2014;42:1178–86. - PubMed
-
- Berney SC, Harrold M, Webb SA, et al. Intensive care unit mobility practices in Australia and New Zealand: a point prevalence study. Crit Care Resusc. 2013;15:260–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
