

Central nervous system histoplasmosis: Multicenter retrospective study on clinical features, diagnostic approach and outcome of treatment
- PMID: 29595679
- PMCID: PMC5895412
- DOI: 10.1097/MD.0000000000010245
Central nervous system histoplasmosis: Multicenter retrospective study on clinical features, diagnostic approach and outcome of treatment
Erratum in
-
Central nervous system histoplasmosis: Multicenter retrospective study on clinical features, diagnostic approach and outcome of treatment: Erratum.Medicine (Baltimore). 2018 Apr;97(16):e0537. doi: 10.1097/MD.0000000000010537. Medicine (Baltimore). 2018. PMID: 29668643 Free PMC article. No abstract available.
Abstract
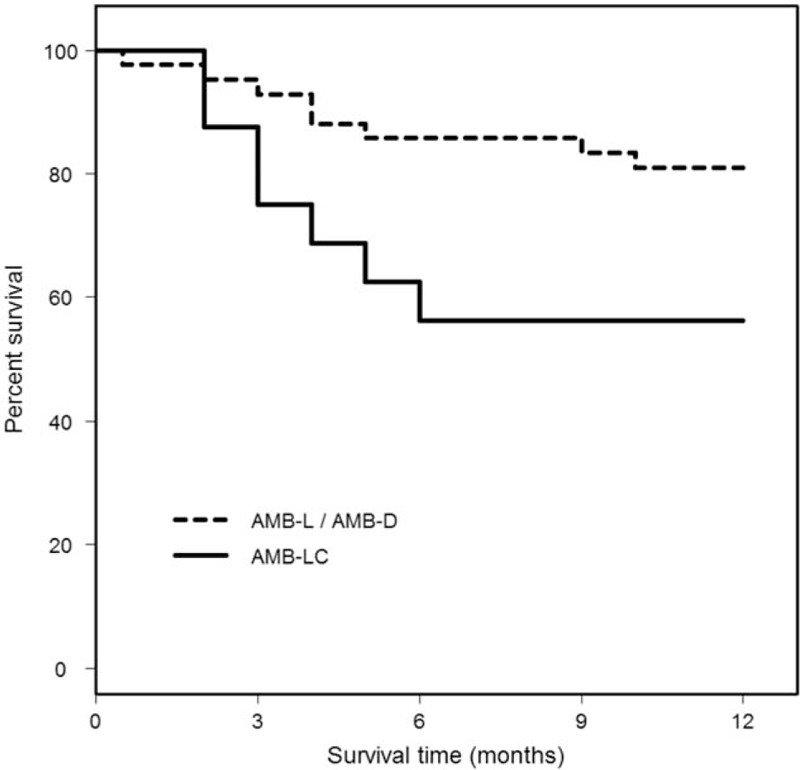
Central nervous system (CNS) involvement occurs in 5 to 10% of individuals with disseminated histoplasmosis. Most experience has been derived from small single center case series, or case report literature reviews. Therefore, a larger study of central nervous system (CNS) histoplasmosis is needed in order to guide the approach to diagnosis, and treatment.A convenience sample of 77 patients with histoplasmosis infection of the CNS was evaluated. Data was collected that focused on recognition of infection, diagnostic techniques, and outcomes of treatment.Twenty nine percent of patients were not immunosuppressed. Histoplasma antigen, or anti-Histoplasma antibodies were detected in the cerebrospinal fluid (CSF) in 75% of patients. One year survival was 75% among patients treated initially with amphotericin B, and was highest with liposomal, or deoxycholate formulations. Mortality was higher in immunocompromised patients, and patients 54 years of age, or older. Six percent of patients relapsed, all of whom had the acquired immunodeficiency syndrome (AIDS), and were poorly adherent with treatment.While CNS histoplasmosis occurred most often in immunocompromised individuals, a significant proportion of patients were previously, healthy. The diagnosis can be established by antigen, and antibody testing of the CSF, and serum, and antigen testing of the urine in most patients. Treatment with liposomal amphotericin B (AMB-L) for at least 1 month; followed by itraconazole for at least 1 year, results in survival among the majority of individuals. Patients should be followed for relapse for at least 1 year, after stopping therapy.
Conflict of interest statement
Potential conflicts of interest: L.J.W is a medical director, and part owner of MiraVista Diagnostics, a company that offers the some of the described tests (antigen and antibody testing) commercially. All other authors report no potential conflicts of interest. All authors have submitted the ICMJE form for disclosure of potential conflicts of interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Wheat LJ, Batteiger BE, Sathapatayavongs B. Histoplasma capsulatum infections of the central nervous system. A clinical review. Medicine (Baltimore) 1990;69:244–60. - PubMed
-
- Schestatsky P, Chedid MF, Amaral OB, et al. Isolated central nervous system histoplasmosis in immunocompetent hosts: a series of 11 cases. Scand J Infect Dis 2006;38:43–8. - PubMed
-
- Nyalakonda H, Albuerne M, Suazo Hernandez LP, et al. Central Nervous System Histoplasmosis in Acquired Immunodeficiency Syndrome. Am J Med Sci 2016;351:177–86. - PubMed
-
- Ellner JJ, Bennett JE. Chronic meningitis. Medicine (Baltimore) 1976;55:341–69. - PubMed
-
- Wheat LJ, Musial CE, Jenny-Avital E. Diagnosis and management of central nervous system histoplasmosis. Clin Infect Dis 2005;40:844–52. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
