

Trends in Physician Payments for Breast Reconstruction
- PMID: 29595721
- PMCID: PMC5880309
- DOI: 10.1097/PRS.0000000000004205
Trends in Physician Payments for Breast Reconstruction
Erratum in
-
Trends in Physician Payments for Breast Reconstruction: Correction.Plast Reconstr Surg. 2018 Sep;142(3):833. doi: 10.1097/PRS.0000000000004972. Plast Reconstr Surg. 2018. PMID: 30148794 No abstract available.
Abstract
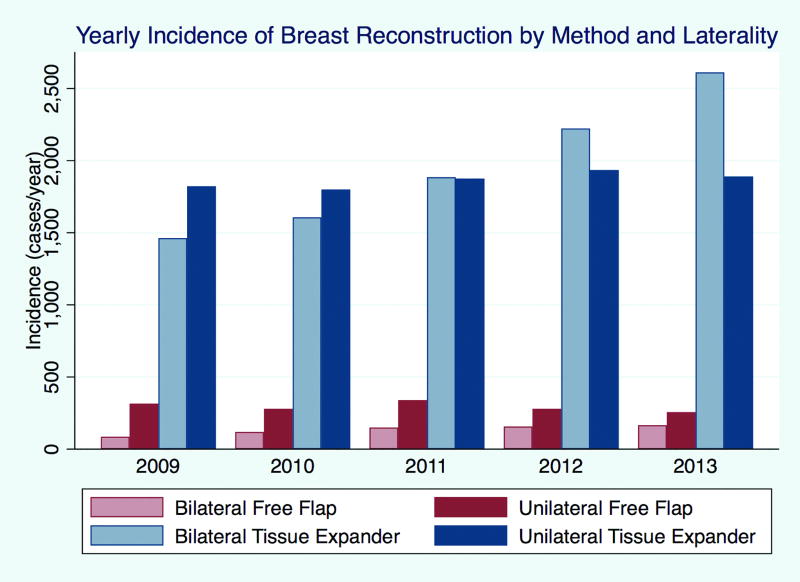
Background: Prosthetic breast reconstruction rates have risen in the United States, whereas autologous techniques have stagnated. Meanwhile, single-institution data demonstrate that physician payments for prosthetic reconstruction are rising, while payments for autologous techniques are unchanged. This study aims to assess payment trends and variation for tissue expander and free flap breast reconstruction.
Methods: The Blue Health Intelligence database was queried from 2009 to 2013, identifying women with claims for breast reconstruction. Trends in the incidence of surgery and physician reimbursement were characterized by method and year using regression models.
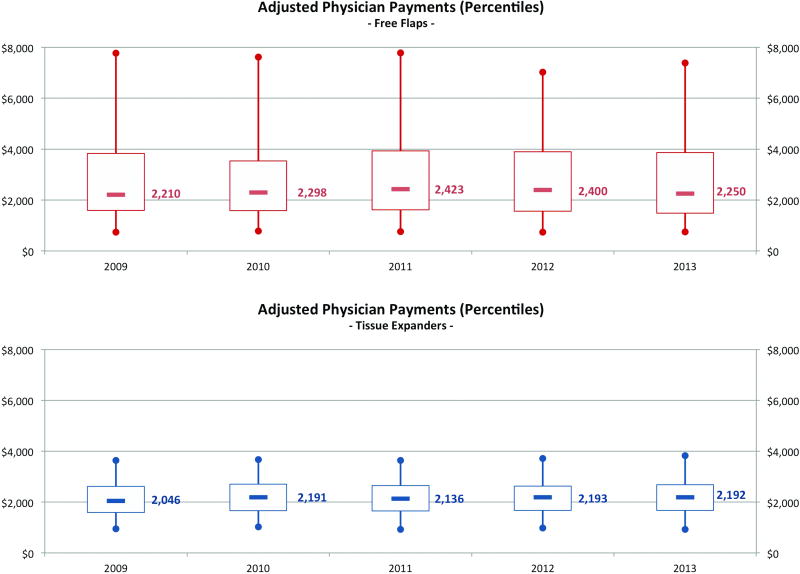
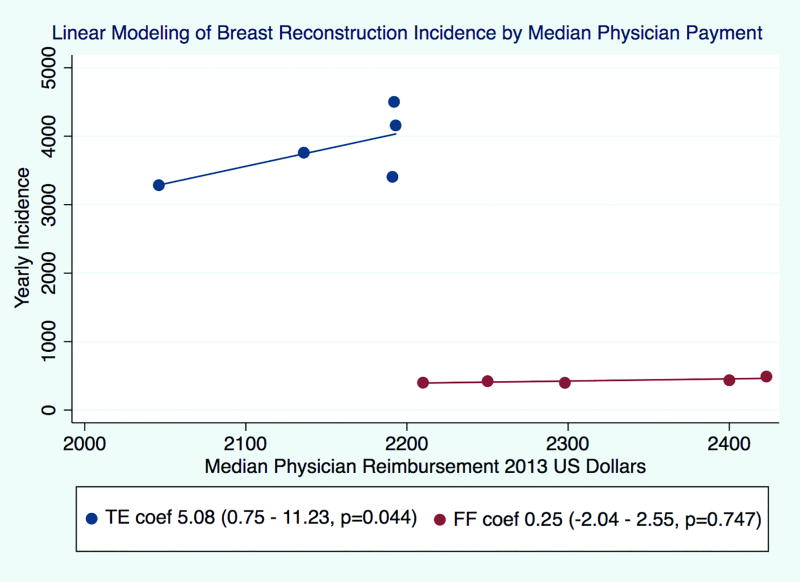
Results: There were 21,259 episodes of breast reconstruction, with a significant rise in tissue expander cases (incidence rate ratio, 1.09; p < 0.001) and an unchanged incidence of free flap cases (incidence rate ratio, 1.02; p = 0.222). Bilateral tissue expander cases reimbursed 1.32 times more than unilateral tissue expanders, whereas bilateral free flaps reimbursed 1.61 times more than unilateral variants. The total growth in adjusted tissue expander mean payments was 6.5 percent (from $2232 to $2378) compared with -1.8 percent (from $3858 to $3788) for free flaps. Linear modeling showed significant increases for tissue expander reimbursements only. Surgeon payments varied more for free flaps (the 25th to 75th percentile interquartile range was $2243 for free flaps versus $987 for tissue expanders).
Conclusions: The incidence of tissue expander cases and reimbursements rose over a period where the incidence of free flap cases and reimbursements plateaued. Reasons for stagnation in free flaps are unclear; however, the opportunity cost of performing this procedure may incentivize the alternative technique. Greater payment variation in autologous reconstruction suggests the opportunity for negotiation with payers.
Figures
Similar articles
-
The Influence of Physician Payments on the Method of Breast Reconstruction: A National Claims Analysis.Plast Reconstr Surg. 2018 Oct;142(4):434e-442e. doi: 10.1097/PRS.0000000000004727. Plast Reconstr Surg. 2018. PMID: 29979366 Free PMC article.
-
Breast reconstruction modality outcome study: a comparison of expander/implants and free flaps in select patients.Plast Reconstr Surg. 2013 May;131(5):928-934. doi: 10.1097/PRS.0b013e3182865977. Plast Reconstr Surg. 2013. PMID: 23629074
-
Impact of Physician Payments on Microvascular Breast Reconstruction: An All-Payer Claim Database Analysis.Plast Reconstr Surg. 2020 Feb;145(2):333-339. doi: 10.1097/PRS.0000000000006453. Plast Reconstr Surg. 2020. PMID: 31985616 Free PMC article.
-
A comparison of acellular dermal matrix to autologous dermal flaps in single-stage, implant-based immediate breast reconstruction: a cost-effectiveness analysis.Plast Reconstr Surg. 2013 May;131(5):953-961. doi: 10.1097/PRS.0b013e3182865a24. Plast Reconstr Surg. 2013. PMID: 23629077 Review.
-
Evolving Approaches to Tissue Expander Design and Application.Plast Reconstr Surg. 2017 Nov;140(5S Advances in Breast Reconstruction):23S-29S. doi: 10.1097/PRS.0000000000003948. Plast Reconstr Surg. 2017. PMID: 29064919 Review.
Cited by
-
Postmastectomy Radiation Therapy (PMRT) before and after 2-Stage Expander-Implant Breast Reconstruction: A Systematic Review.Medicina (Kaunas). 2019 May 29;55(6):226. doi: 10.3390/medicina55060226. Medicina (Kaunas). 2019. PMID: 31146506 Free PMC article.
-
A Retrospective Dosimetric Analysis of the New ESTRO-ACROP Target Volume Delineation Guidelines for Postmastectomy Volumetric Modulated Arc Therapy After Implant-Based Immediate Breast Reconstruction.Front Oncol. 2020 Oct 20;10:578921. doi: 10.3389/fonc.2020.578921. eCollection 2020. Front Oncol. 2020. PMID: 33194701 Free PMC article.
-
An Analysis of Procedural Medicare Reimbursement Rates in Hand Surgery: 2000 to 2019.Hand (N Y). 2022 Nov;17(6):1207-1213. doi: 10.1177/1558944721990807. Epub 2021 Feb 25. Hand (N Y). 2022. PMID: 33631979 Free PMC article.
-
Complications, Costs, and Healthcare Resource Utilization After Staged, Delayed, and Immediate Free-Flap Breast Reconstruction: A Longitudinal, Claims-Based Analysis.Ann Surg Oncol. 2023 Apr;30(4):2534-2549. doi: 10.1245/s10434-022-12896-0. Epub 2022 Dec 6. Ann Surg Oncol. 2023. PMID: 36474094 Free PMC article.
-
Immediate versus secondary DIEP flap breast reconstruction: a multicenter outcome study.Arch Gynecol Obstet. 2020 Dec;302(6):1451-1459. doi: 10.1007/s00404-020-05779-w. Epub 2020 Sep 7. Arch Gynecol Obstet. 2020. PMID: 32895743 Free PMC article.
References
-
- Albornoz CR, Bach PB, Mehrara BJ, Disa JJ, Pusic AL, McCarthy CM, et al. A paradigm shift in U.S. Breast reconstruction: increasing implant rates. Plast Reconstr Surg. 2013 Jan;131(1):15–23. - PubMed
-
- Albornoz CR, Cordeiro PG, Pusic AL, McCarthy CM, Mehrara BJ, Disa JJ, et al. Diminishing relative contraindications for immediate breast reconstruction: a multicenter study. J Am Coll Surg. 2014 Oct;219(4):788–95. - PubMed
-
- [cited 2017 Apr 21];Blue Health Intelligence [Internet] Available from: https://bluehealthintelligence.com/markets/life-sciences/index.html.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
