

A Dedicated Acute Pain Service Is Associated With Reduced Postoperative Opioid Requirements in Patients Undergoing Cytoreductive Surgery With Hyperthermic Intraperitoneal Chemotherapy
- PMID: 29596098
- PMCID: PMC6135471
- DOI: 10.1213/ANE.0000000000003342
A Dedicated Acute Pain Service Is Associated With Reduced Postoperative Opioid Requirements in Patients Undergoing Cytoreductive Surgery With Hyperthermic Intraperitoneal Chemotherapy
Abstract
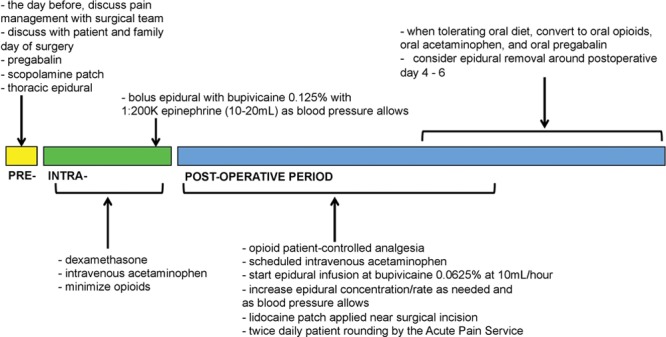
Background: The Acute Pain Service (APS) was initially introduced to optimize multimodal postoperative pain control. The aim of this study was to evaluate the association between the implementation of an APS and postoperative pain management and outcomes for patients undergoing cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CRS-HIPEC).
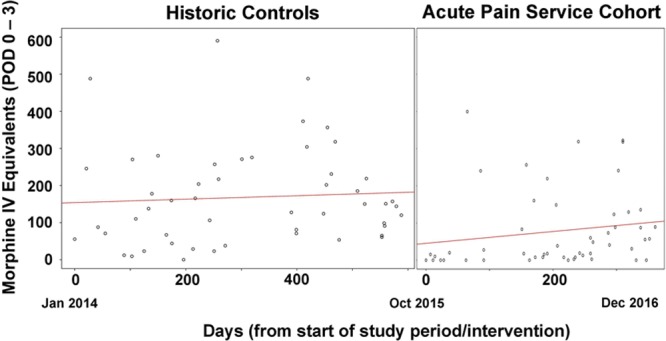
Methods: In this propensity-matched retrospective cohort study, we performed a before-after study without a concurrent control group. Outcomes were compared among patients undergoing CRS-HIPEC when APS was implemented versus historical controls (non-APS). The primary objective was to determine if there was a decrease in median total opioid consumption during postoperative days 0-3 among patients managed by the APS. Secondary outcomes included opioid consumption on each postoperative day (0-6), time to ambulation, time to solid intake, and hospital length of stay.
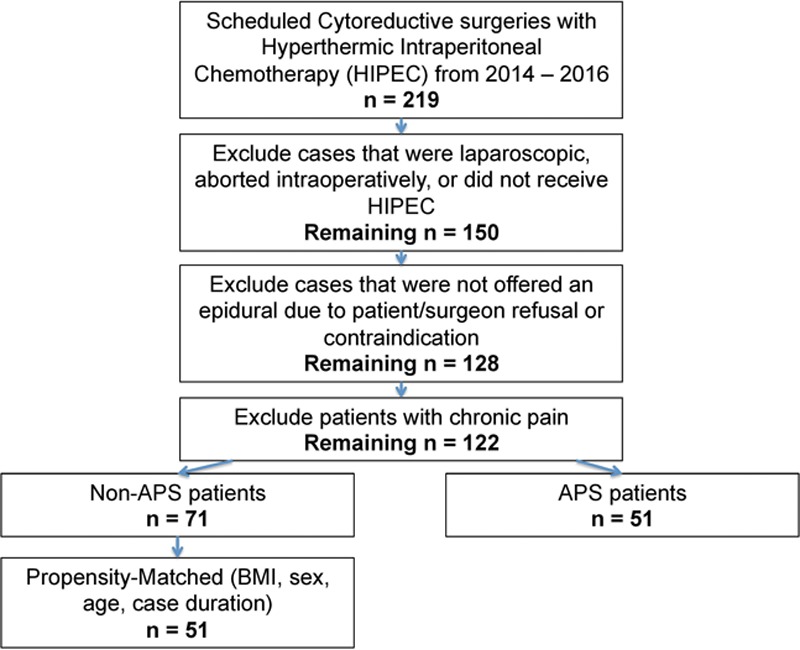
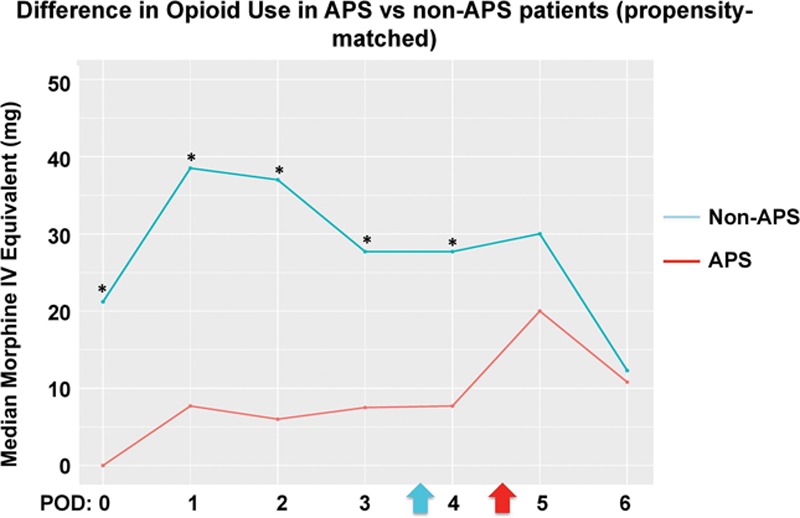
Results: After exclusion, there were a total of 122 patients, of which 51 and 71 were in the APS and non-APS cohort, respectively. Between propensity-matched groups, the median (quartiles) total opioid consumption during postoperative days 0-3 was 27.5 mg intravenous morphine equivalents (MEQs) (7.6-106.3 mg MEQs) versus 144.0 mg MEQs (68.9-238.3 mg MEQs), respectively. The median difference was 80.8 mg MEQs (95% confidence interval, 46.1-124.0; P < .0001). There were statistically significant decreases in time to ambulation and time to solid diet intake in the APS cohort.
Conclusions: After implementing the APS, CRS-HIPEC patients had decreased opioid consumption by >50%, as well as shorter time to ambulation and time to solid intake. Implementation of an APS may improve outcomes in CRS-HIPEC patients.
Conflict of interest statement
Conflicts of Interest: See Disclosures at the end of the article.
Figures
Comment in
-
Optimal Organization of Acute Pain Services: At the Confluence of Semantics, Logistics, and Economics.Anesth Analg. 2018 Oct;127(4):808-810. doi: 10.1213/ANE.0000000000003367. Anesth Analg. 2018. PMID: 30216281 No abstract available.
-
Questions About the Study by Said Et Al.Anesth Analg. 2019 Mar;128(3):e50. doi: 10.1213/ANE.0000000000004010. Anesth Analg. 2019. PMID: 30676347 No abstract available.
-
In Response.Anesth Analg. 2019 Mar;128(3):e51. doi: 10.1213/ANE.0000000000004011. Anesth Analg. 2019. PMID: 30676352 No abstract available.
References
-
- Gandhi K, Heitz JW, Viscusi ER. Challenges in acute pain management. Anesthesiol Clin. 2011;29:291–309.. - PubMed
-
- Lucas CE, Vlahos AL, Ledgerwood AM. Kindness kills: the negative impact of pain as the fifth vital sign. J Am Coll Surg. 2007;205:101–107.. - PubMed
-
- Oderda GM, Said Q, Evans RS, et al. Opioid-related adverse drug events in surgical hospitalizations: impact on costs and length of stay. Ann Pharmacother. 2007;41:400–406.. - PubMed
-
- Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003;97:534–540.. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
