

Survival in Locally Advanced Pancreatic Cancer After Neoadjuvant Therapy and Surgical Resection
- PMID: 29596120
- PMCID: PMC6985003
- DOI: 10.1097/SLA.0000000000002753
Survival in Locally Advanced Pancreatic Cancer After Neoadjuvant Therapy and Surgical Resection
Abstract
Objective: The aim of the study was to identify the survival of patients with locally advanced pancreatic cancer (LAPC) and assess the effect of surgical resection after neoadjuvant therapy on patient outcomes.
Background: An increasing number of LAPC patients who respond favorably to neoadjuvant therapy undergo surgical resection. The impact of surgery on patient survival is largely unknown.
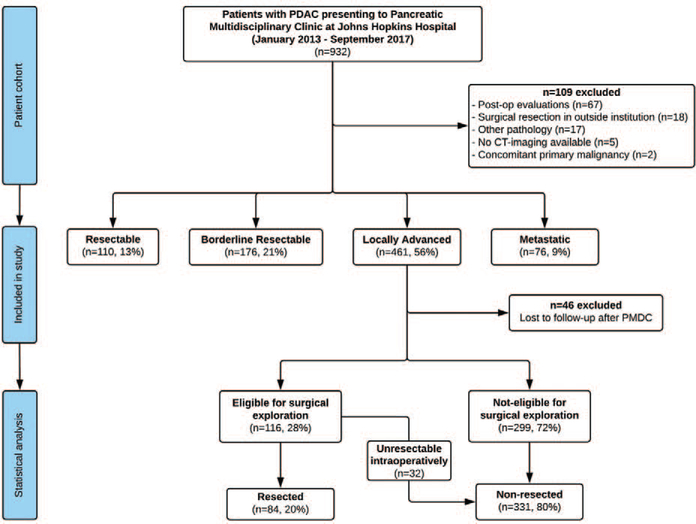
Materials and methods: All LAPC patients who presented to the institutional pancreatic multidisciplinary clinic (PMDC) from January 2013 to September 2017 were included in the study. Demographics and clinical data on neoadjuvant treatment and surgical resection were documented. Primary tumor resection rates after neoadjuvant therapy and overall survival (OS) were the primary study endpoints.
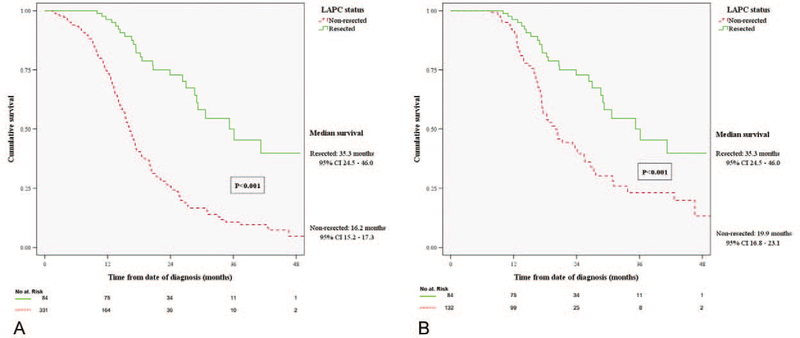
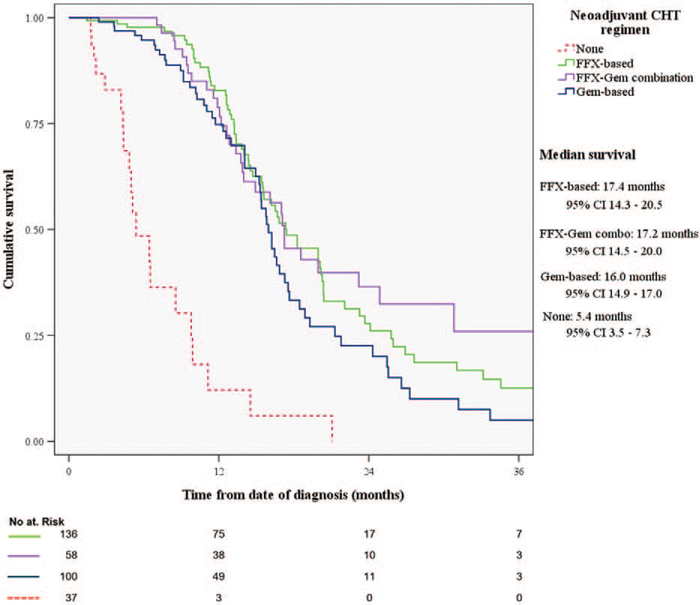
Results: A total of 415 LAPC patients were included in the study. Stratification of neoadjuvant therapy in FOLFIRINOX-based, gemcitabine-based, and combination of the two, and subsequent outcome comparison did not demonstrate significant differences in OS of 331 non-resected LAPC patients (P = 0.134). Eighty-four patients underwent resection of the primary tumor (20%), after a median duration of 5 months of neoadjuvant therapy. FOLFIRINOX-based therapy and stereotactic body radiation therapy correlated with increased probability of resection (P = 0.006). Resected patients had better performance status, smaller median tumor size (P = 0.029), and lower median CA19-9 values (P < 0.001) at PMDC. Patients who underwent surgical resection had significant higher median OS compared with those who did not (35.3 vs 16.3 mo, P < 0.001). The difference remained significant when non-resected patients were matched for time of neoadjuvant therapy (19.9 mo, P < 0.001).
Conclusions: Surgical resection of LAPC after neoadjuvant therapy is feasible in a highly selected cohort of patients (20%) and is associated with significantly longer median overall survival.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Comment in
-
Locally advanced pancreatic cancer: staging, operability, and the importance of multimodality therapy.Hepatobiliary Surg Nutr. 2020 Aug;9(4):497-500. doi: 10.21037/hbsn.2019.11.26. Hepatobiliary Surg Nutr. 2020. PMID: 32832502 Free PMC article. No abstract available.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. 2017;67:7–30. - PubMed
-
- Rahib L, Smith BD, Aizenberg R, et al. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74:2913–2921. - PubMed
-
- Balaban EP, Mangu PB, Khorana AA, et al. Locally advanced, unresectable pancreatic cancer: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2016;34:2654–2668. - PubMed
-
- Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364:1817–1825. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
