

Changes in Lumbar Endplate Area and Concavity Associated With Disc Degeneration
- PMID: 29596278
- PMCID: PMC6145136
- DOI: 10.1097/BRS.0000000000002657
Changes in Lumbar Endplate Area and Concavity Associated With Disc Degeneration
Abstract
Study design: Retrospective image-based analysis.
Objective: To measure endplate three-dimensional (3D) geometry, endplate changes in vivo and to investigate correlations between disc degeneration and endplate 3D geometry dependent on symptoms of low back pain (LBP).
Summary of background data: It has been hypothesized that alteration of load transmission from the nucleus pulposus to the annulus fibrosus affects vertebral endplate geometry.
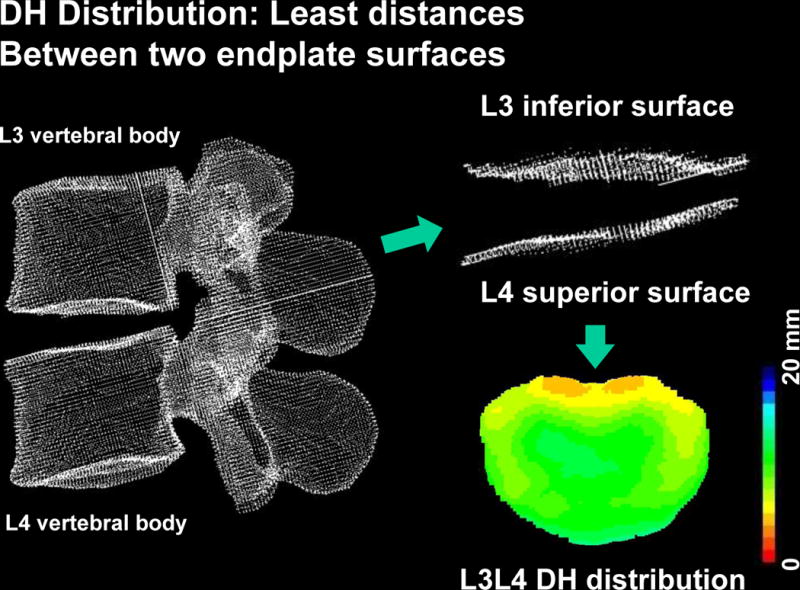
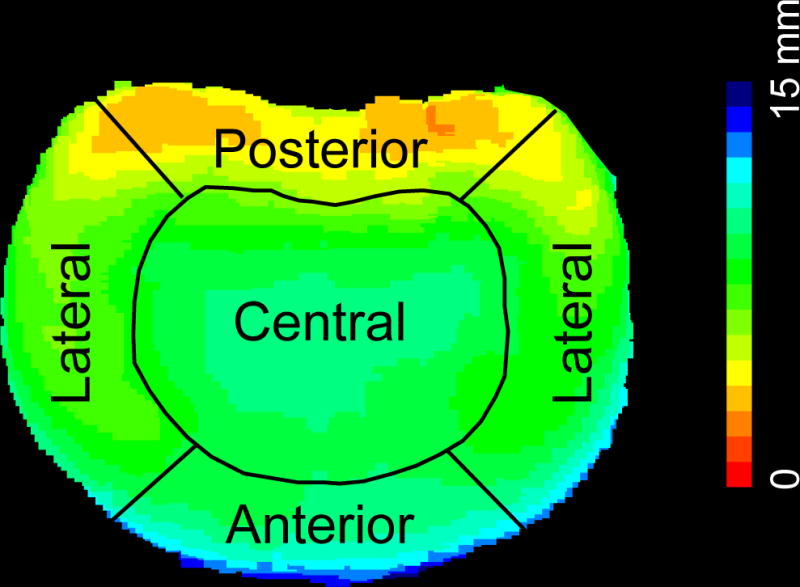
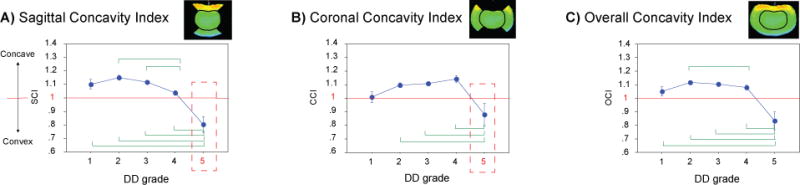
Methods: 3D surface models of inferior/superior lumbar endplates were created from computed tomography scans of n = 92 volunteers with and without LBP. Disc degeneration was evaluated using Pfirrmann scale. Concavity in both coronal and sagittal planes was assessed with the Concavity Index (unitless; larger than 1: concave; flat: 1; and less than 1: convex, respectively). Endplate area and disc height distribution were computed and the effects from demographics and spinal degeneration were sought with an analysis of variance model.
Results: Both sagittal and coronal planes revealed significantly decreased concavity in those with terminal grade 5 disc degeneration (mean 0.833 ± 0.235) compared to the other grades in the cohort. Older subjects presented with larger endplate areas than the younger subjects (P = 0.0148) at L4-S1. Overall, symptomatic subjects had significantly larger endplate areas (P = 0.022), especially at the lower lumbar levels (P < 0.001). Analysis of variance showed that sex, disc level, disc degeneration grade, and disc height reached significance (P < 0.0001) as influential parameters in both Concavity Index cases.
Conclusion: With advancing intervertebral disc degeneration, endplates become more convex over time in both sagittal and coronal planes. Our findings implicate the endplate changes with advancing disc degeneration in the shift in load transmission from the nucleus pulposus to the annulus fibrosus, resulting in changes within the curvature of the endplates. This is also the first study to describe the direct impact of age, sex, and LBP on vertebral endplate anatomy.
Level of evidence: 5.
Figures



References
-
- Mok FPS, Samartzis D, Karppinen J, Fong DYT, Luk KDK, Cheung KMC. Modic changes of the lumbar spine: prevalence, risk factors, and association with disc degeneration and low back pain in a large-scale population-based cohort. Spine J. 2016;16(1):32–41. doi: 10.1016/j.spinee.2015.09.060. - DOI - PubMed
-
- White AA, III, Panjabi MM. Clinical Biomechanics of the Spine. 2nd. Philadelphia: Lippincott; 1990.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
