

Community-based MDR-TB care project improves treatment initiation in patients diagnosed with MDR-TB in Myanmar
- PMID: 29596434
- PMCID: PMC5875775
- DOI: 10.1371/journal.pone.0194087
Community-based MDR-TB care project improves treatment initiation in patients diagnosed with MDR-TB in Myanmar
Abstract
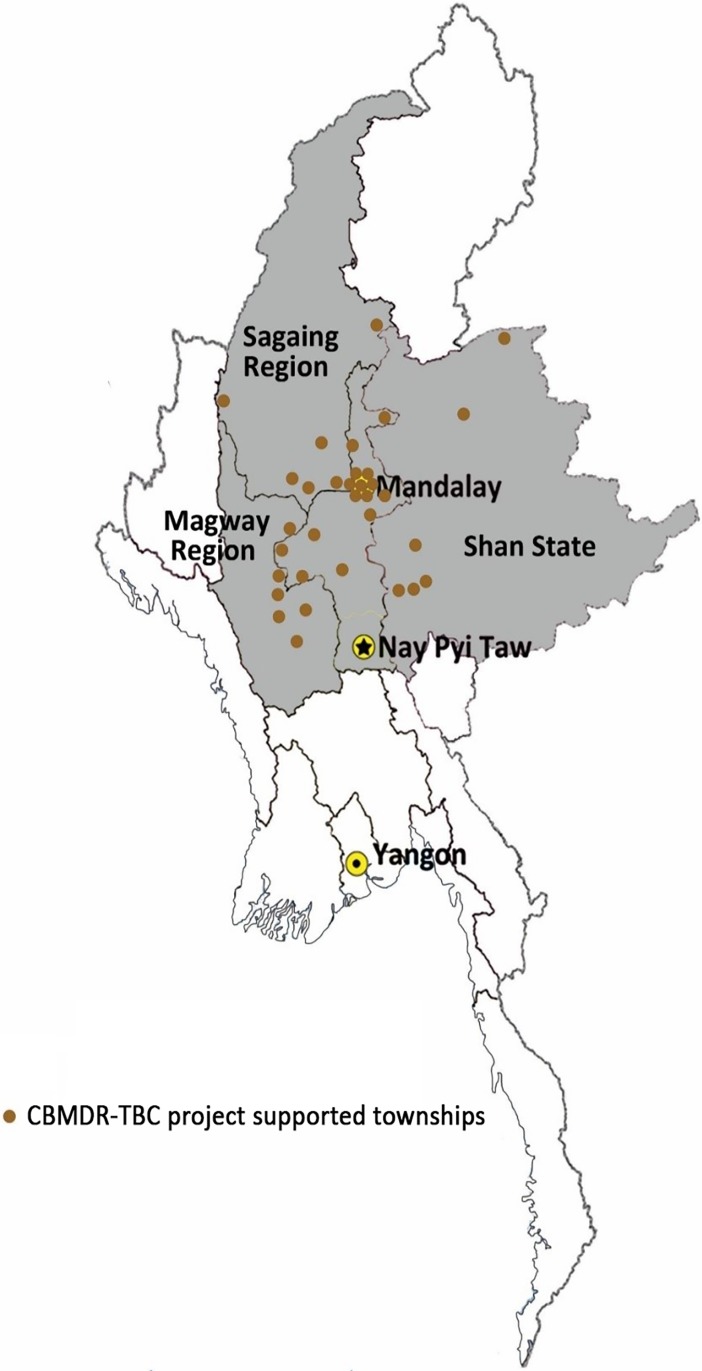
Background: The Union in collaboration with national TB programme (NTP) started the community-based MDR-TB care (CBMDR-TBC) project in 33 townships of upper Myanmar to improve treatment initiation and treatment adherence. Patients with MDR-TB diagnosed/registered under NTP received support through the project staff, in addition to the routine domiciliary care provided by NTP staff. Each township had a project nurse exclusively for MDR-TB and 30 USD per month (max. for 4 months) were provided to the patient as a pre-treatment support.
Objectives: To assess whether CBMDR-TBC project's support improved treatment initiation.
Methods: In this cohort study (involving record review) of all diagnosed MDR-TB between January 2015 and June 2016 in project townships, CBMDR-TBC status was categorized as "receiving support" if date of project initiation in patient's township was before the date of diagnosis and "not receiving support", if otherwise. Cox proportional hazards regression (censored on 31 Dec 2016) was done to identify predictors of treatment initiation.
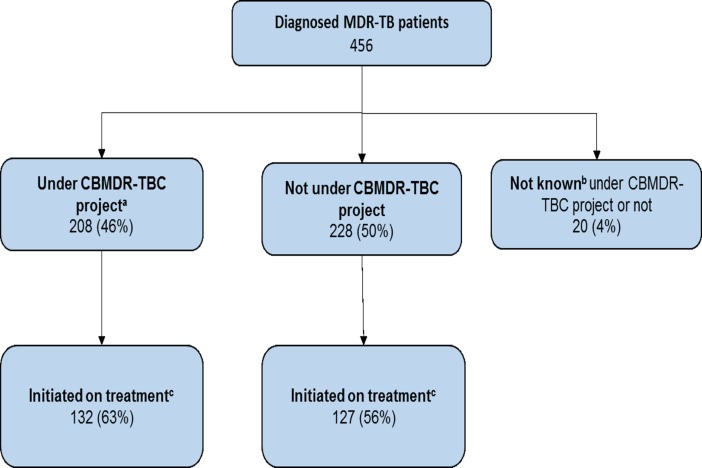
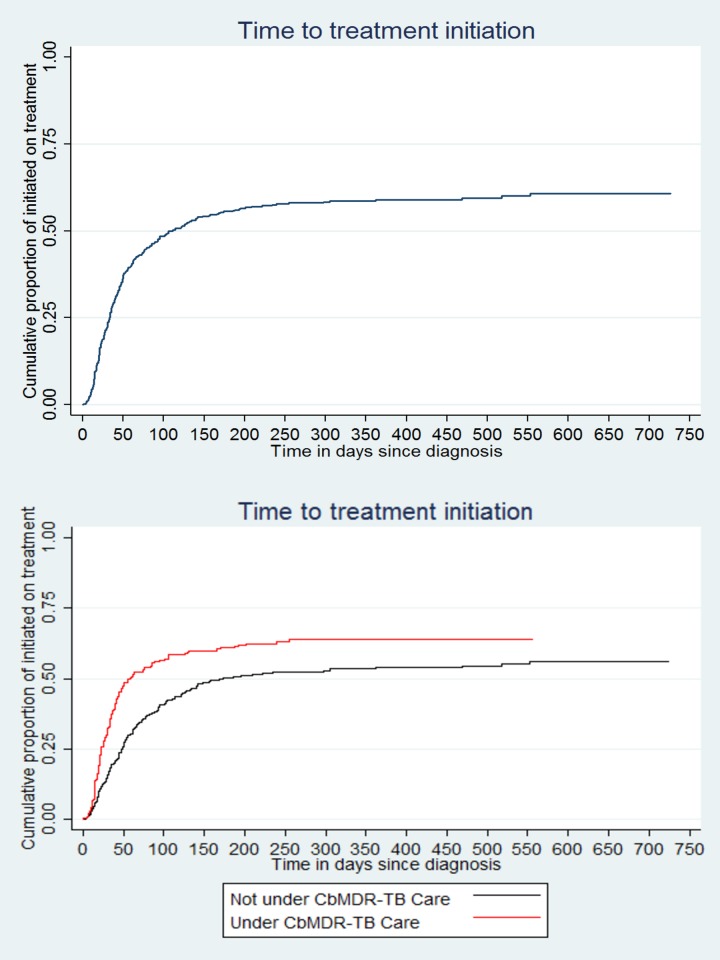
Results: Of 456 patients, 57% initiated treatment: 64% and 56% among patients "receiving support (n = 208)" and "not receiving support (n = 228)" respectively (CBMDR-TBC status was not known in 20 (4%) patients due to missing diagnosis dates). Among those initiated on treatment (n = 261), median (IQR) time to initiate treatment was 38 (20, 76) days: 31 (18, 50) among patients "receiving support" and 50 (26,101) among patients "not receiving support". After adjusting other potential confounders (age, sex, region, HIV, past history of TB treatment), patients "receiving support" had 80% higher chance of initiating treatment [aHR (0.95 CI): 1.8 (1.3, 2.3)] when compared to patients "not receiving support". In addition, age 15-54 years, previous history of TB and being HIV negative were independent predictors of treatment initiation.
Conclusion: Receiving support under CBMDR-TBC project improved treatment initiation: it not only improved the proportion initiated but also reduced time to treatment initiation. We also recommend improved tracking of all diagnosed patients as early as possible.
Conflict of interest statement
Figures
Similar articles
-
Patients with MDR-TB on domiciliary care in programmatic settings in Myanmar: Effect of a support package on preventing early deaths.PLoS One. 2017 Dec 20;12(12):e0187223. doi: 10.1371/journal.pone.0187223. eCollection 2017. PLoS One. 2017. PMID: 29261669 Free PMC article.
-
High treatment success rate among multidrug-resistant tuberculosis patients in Myanmar, 2012-2014: a retrospective cohort study.Trans R Soc Trop Med Hyg. 2017 Sep 1;111(9):410-417. doi: 10.1093/trstmh/trx074. Trans R Soc Trop Med Hyg. 2017. PMID: 29351672
-
Delay in diagnosis and treatment among adult multidrug resistant tuberculosis patients in Yangon Regional Tuberculosis Center, Myanmar: a cross-sectional study.BMC Health Serv Res. 2018 Nov 20;18(1):878. doi: 10.1186/s12913-018-3715-4. BMC Health Serv Res. 2018. PMID: 30458776 Free PMC article.
-
Delay in treatment initiation and treatment outcomes among adult patients with multidrug-resistant tuberculosis at Yangon Regional Tuberculosis Centre, Myanmar: A retrospective study.PLoS One. 2018 Dec 31;13(12):e0209932. doi: 10.1371/journal.pone.0209932. eCollection 2018. PLoS One. 2018. PMID: 30596734 Free PMC article. Clinical Trial.
-
Predictors of cure among HIV co-infected multidrug-resistant TB patients at Sizwe Tropical Disease Hospital Johannesburg, South Africa.Trans R Soc Trop Med Hyg. 2015 May;109(5):340-8. doi: 10.1093/trstmh/trv025. Epub 2015 Mar 18. Trans R Soc Trop Med Hyg. 2015. PMID: 25787727 Review.
Cited by
-
Contact Investigation of Multidrug-Resistant Tuberculosis Patients: A Mixed-Methods Study from Myanmar.Trop Med Infect Dis. 2019 Dec 26;5(1):3. doi: 10.3390/tropicalmed5010003. Trop Med Infect Dis. 2019. PMID: 31887995 Free PMC article.
-
Attrition and delays before treatment initiation among patients with MDR-TB in China (2006-13): Magnitude and risk factors.PLoS One. 2019 Apr 8;14(4):e0214943. doi: 10.1371/journal.pone.0214943. eCollection 2019. PLoS One. 2019. PMID: 30958841 Free PMC article. Clinical Trial.
-
Impact of GxAlert on the management of rifampicin-resistant tuberculosis patients, Port Moresby, Papua New Guinea.Public Health Action. 2019 Sep 21;9(Suppl 1):S19-S24. doi: 10.5588/pha.18.0067. Public Health Action. 2019. PMID: 31579645 Free PMC article.
-
Adherence to Multidrug Resistant Tuberculosis Treatment and Case Management in Chongqing, China - A Mixed Method Research Study.Infect Drug Resist. 2021 Mar 15;14:999-1012. doi: 10.2147/IDR.S293583. eCollection 2021. Infect Drug Resist. 2021. PMID: 33758516 Free PMC article.
-
Factors predicting self-report adherence (SRA) behaviours among DS-TB patients under the "Integrated model": a survey in Southwest China.BMC Infect Dis. 2022 Mar 1;22(1):201. doi: 10.1186/s12879-022-07208-6. BMC Infect Dis. 2022. PMID: 35232384 Free PMC article.
References
-
- World Health Organization (WHO). Global Tuberculosis Report 2016. Geneva, Switzerland; 2016. doi:ISBN 978 92 4 156539 4
-
- Hossain ST, Isaakidis P, Sagili KD, Islam S, Islam MA, Shewade HD, et al. The Multi-Drug Resistant Tuberculosis Diagnosis and Treatment Cascade in Bangladesh. PLoS One. 2015;10: e0129155 doi: 10.1371/journal.pone.0129155 - DOI - PMC - PubMed
-
- Singla N, Satyanarayana S, Sachdeva KS, Van den Bergh R, Reid T, Tayler-Smith K, et al. Impact of Introducing the Line Probe Assay on Time to Treatment Initiation of MDR-TB in Delhi, India. Sola C, editor. PLoS One. 2014;9: 5 doi: 10.1371/journal.pone.0102989 - DOI - PMC - PubMed
-
- Cox H, Dickson-Hall L, Ndjeka N, van’t Hoog A, Grant A, Cobelens F, et al. Delays and loss to follow-up before treatment of drug-resistant tuberculosis following implementation of Xpert MTB/RIF in South Africa: A retrospective cohort study. Suthar AB, editor. PLOS Med. South African National Department of Health; 2017;14: 19 doi: 10.1371/journal.pmed.1002238 - DOI - PMC - PubMed
-
- Harris RC, Grandjean L, Martin LJ, Miller AJP, Nkang J-EN, Allen V, et al. The effect of early versus late treatment initiation after diagnosis on the outcomes of patients treated for multidrug-resistant tuberculosis: a systematic review. BMC Infect Dis. 2016;16: 193 doi: 10.1186/s12879-016-1524-0 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
