

Potential geographic "hotspots" for drug-injection related transmission of HIV and HCV and for initiation into injecting drug use in New York City, 2011-2015, with implications for the current opioid epidemic in the US
- PMID: 29596464
- PMCID: PMC5875800
- DOI: 10.1371/journal.pone.0194799
Potential geographic "hotspots" for drug-injection related transmission of HIV and HCV and for initiation into injecting drug use in New York City, 2011-2015, with implications for the current opioid epidemic in the US
Abstract
Objective: We identified potential geographic "hotspots" for drug-injecting transmission of HIV and hepatitis C virus (HCV) among persons who inject drugs (PWID) in New York City. The HIV epidemic among PWID is currently in an "end of the epidemic" stage, while HCV is in a continuing, high prevalence (> 50%) stage.
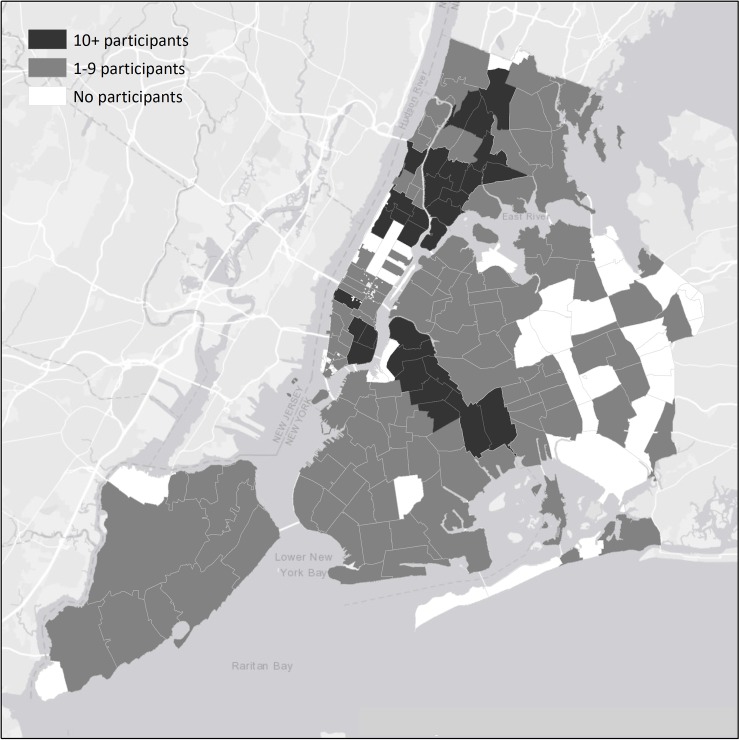
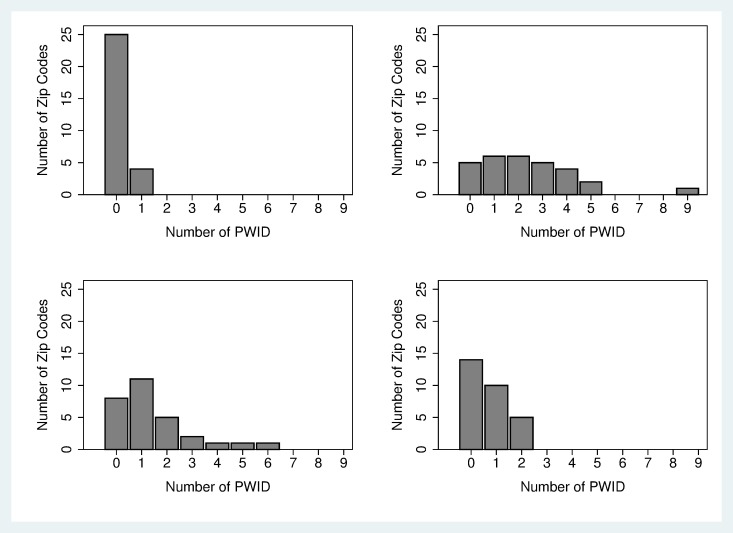
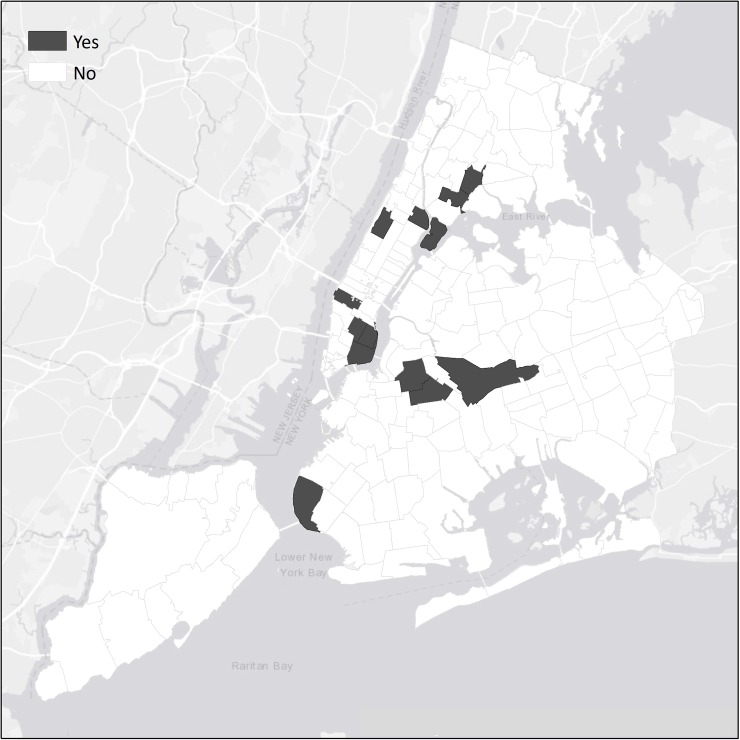
Methods: We recruited 910 PWID entering Mount Sinai Beth Israel substance use treatment programs from 2011-2015. Structured interviews and HIV/ HCV testing were conducted. Residential ZIP codes were used as geographic units of analysis. Potential "hotspots" for HIV and HCV transmission were defined as 1) having relatively large numbers of PWID 2) having 2 or more HIV (or HCV) seropositive PWID reporting transmission risk-passing on used syringes to others, and 3) having 2 or more HIV (or HCV) seronegative PWID reporting acquisition risk-injecting with previously used needles/syringes. Hotspots for injecting drug use initiation were defined as ZIP codes with 5 or more persons who began injecting within the previous 6 years.
Results: Among PWID, 96% injected heroin, 81% male, 34% White, 15% African-American, 47% Latinx, mean age 40 (SD = 10), 7% HIV seropositive, 62% HCV seropositive. Participants resided in 234 ZIP codes. No ZIP codes were identified as potential hotspots due to small numbers of HIV seropositive PWID reporting transmission risk. Four ZIP codes were identified as potential hotspots for HCV transmission. 12 ZIP codes identified as hotspots for injecting drug use initiation.
Discussion: For HIV, the lack of potential hotspots is further validation of widespread effectiveness of efforts to reduce injecting-related HIV transmission. Injecting-related HIV transmission is likely to be a rare, random event. HCV prevention efforts should include focus on potential hotspots for transmission and on hotspots for initiation into injecting drug use. We consider application of methods for the current opioid epidemic in the US.
Conflict of interest statement
Figures

References
-
- Levy MZ, Bowman NM, Kawai V, Plotkin JB, Waller LA, Cabrera L, et al. Spatial patterns in discordant diagnostic test results for Chagas disease: links to transmission hotspots. Clin Infect Dis. 2009. April 15;48(8):1104–6. doi: 10.1086/597464 - DOI - PMC - PubMed
-
- Paull SH, Song S, McClure KM, Sackett LC, Kilpatrick AM, Johnson PT. From superspreaders to disease hotspots: linking transmission across hosts and space. Front Ecol Environ. 2012. Mar January;10(2):75–82. doi: 10.1890/110111 - DOI - PMC - PubMed
-
- Kauhl B, Heil J, Hoebe CJ, Schweikart J, Krafft T, Dukers-Muijrers NH. The spatial distribution of hepatitis C virus infections and associated determinants—An application of a geographically weighted poisson regression for evidence-based screening interventions in hotspots. PLoS One. 2015. September 9;10(9):e0135656 doi: 10.1371/journal.pone.0135656 - DOI - PMC - PubMed
-
- Meyers DJ, Hood ME, Stopka TJ. HIV and hepatitis C mortality in Massachusetts, 2002–2011: spatial cluster and trend analysis of HIV and HCV using multiple cause of death. PLoS One. 2014. December 11;9(12):e114822 doi: 10.1371/journal.pone.0114822 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
