

Influenza virus: 16 years' experience of clinical epidemiologic patterns and associated infection factors in hospitalized children in Argentina
- PMID: 29596527
- PMCID: PMC5875855
- DOI: 10.1371/journal.pone.0195135
Influenza virus: 16 years' experience of clinical epidemiologic patterns and associated infection factors in hospitalized children in Argentina
Abstract
Background: Influenza is an important cause of acute lower respiratory tract infection (aLRTI), hospitalization, and mortality in children. This study aimed to describe the clinical and epidemiologic patterns and infection factors associated with influenza, and compare case features of influenza A and B.
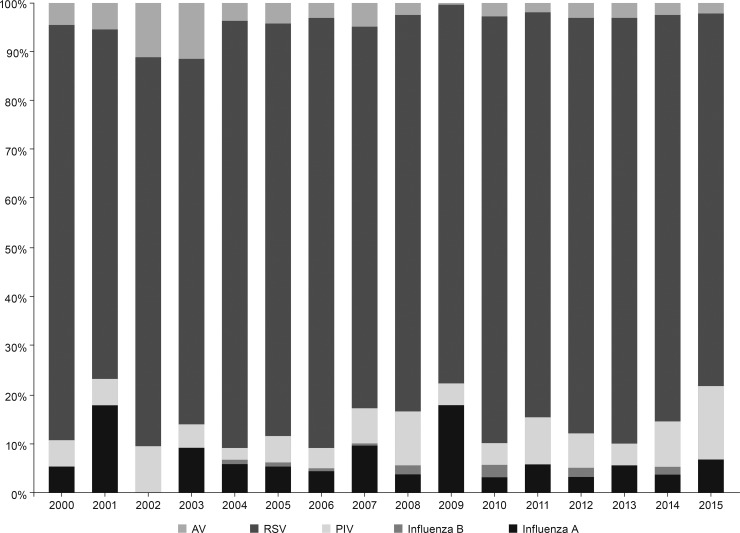
Methods: In a prospective, cross-sectional study, patients admitted for aLRTI, between 2000 and 2015, were tested for respiratory syncytial virus, adenovirus, influenza, or parainfluenza, and confirmed by fluorescent antibody (FA) or real-time polymerase chain reaction (RT-PCR) assay of nasopharyngeal aspirates.
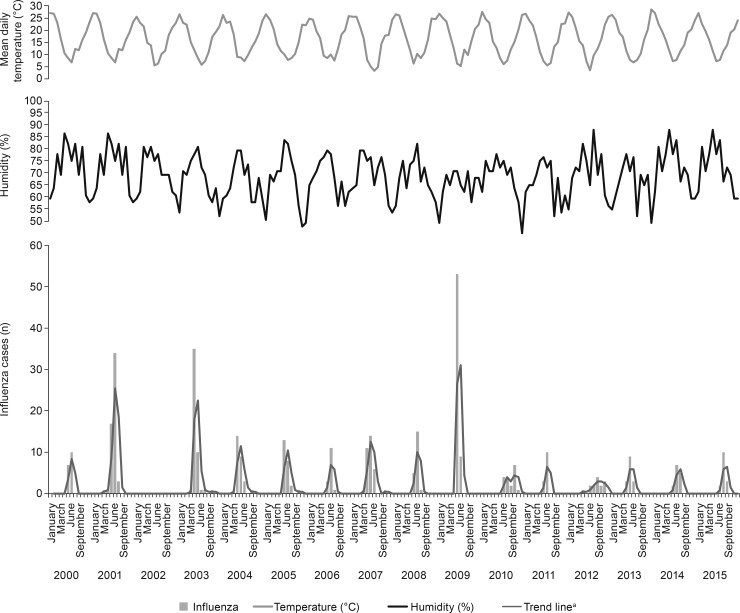
Results: Of 14,044 patients, 37.7% (5290) had FA- or RT-PCR-confirmed samples that identified influenza in 2.8% (394/14,044; 91.4% [360] influenza A, 8.6% [34] influenza B) of cases. Influenza frequency followed a seasonal epidemic pattern (May-July, the lowest average temperature months). The median age of cases was 12 months (interquartile range: 6-21 months); 56.1% (221/394) of cases were male. Consolidated pneumonia was the most frequent clinical presentation (56.9%; 224/394). Roughly half (49.7%; 196/394) of all cases had previous respiratory admissions; 9.4% (37/394) were re-admissions; 61.5% (241/392) had comorbidities; 26.2% (102/389) had complications; 7.8% (30/384) had nosocomial infections. The average case fatality rate was 2.1% (8/389). Chronic neurologic disease was significantly higher in influenza B cases compared to influenza A cases (p = 0.030). The independent predictors for influenza were: age ≥6 months, odds ratio (OR): 1.88 (95% confidence interval [CI]: 1.44-2.45); p<0.001; presence of chronic neurologic disease, OR: 1.48 (95% CI: 1.01-2.17); p = 0.041; previous respiratory admissions, OR: 1.71 (95% CI: 1.36-2.14); p<0.001; re-admissions, OR: 1.71 (95% CI: 1.17-2.51); p = 0.006; clinical pneumonia, OR: 1.50 (95% CI: 1.21-1.87); p<0.001; immunodeficiency, OR: 1.87 (95% CI: 1.15-3.05); p = 0.011; cystic fibrosis, OR: 4.42 (95% CI: 1.29-15.14); p = 0.018.
Conclusion: Influenza showed an epidemic seasonal pattern (May-July), with higher risk in children ≥6 months, or with pneumonia, previous respiratory admissions, or certain comorbidities.
Conflict of interest statement
Figures
References
-
- World Health Organization. Influenza (Seasonal). Factsheet No 211. Available from: http://www.who.int/mediacentre/factsheets/fs211/en/
-
- De Kirchner CEF. Abordaje Integral de las Infecciones Respiratorias Agudas: Guia Para el Equipo de Salud. Dirección de Epidemiología-Ministerio de Salud de la Nación. Available from: http://www.msal.gov.ar/cuidados-invierno/abordaje-integral-de-las-infecc...
-
- Arango AE, Jaramillo S, Perez J, Ampuero JS, Espinal D, Donado J, et al. Influenza-like illness sentinel surveillance in one hospital in Medellin, Colombia. 2007–2012. Influenza Other Respir Viruses. 2015;9(1): 1–13. doi: 10.1111/irv.12271 - DOI - PMC - PubMed
-
- McMorrow ML, Emukule GO, Njuguna HN, Bigogo G, Montgomery JM, Nyawanda B, et al. The unrecognized burden of influenza in young Kenyan children, 2008–2012. PLoS One. 2015;10(9): e0138272 doi: 10.1371/journal.pone.0138272 - DOI - PMC - PubMed
-
- Neuzil KM, Mellen BG, Wright PF, Mitchel EF Jr., Griffin MR. The effect of influenza on hospitalizations, outpatient visits, and courses of antibiotics in children. N Engl J Med. 2000;342(4): 225–231. doi: 10.1056/NEJM200001273420401 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
