

Preoperative Facial Nerve Mapping to Plan and Guide Pediatric Facial Vascular Anomaly Resection
- PMID: 29596549
- PMCID: PMC5876811
- DOI: 10.1001/jamaoto.2018.0054
Preoperative Facial Nerve Mapping to Plan and Guide Pediatric Facial Vascular Anomaly Resection
Abstract
Importance: Facial vascular anomalies are surgical challenges due to their vascularity and facial nerve distortion. To assist facial vascular anomaly surgical treatment, presurgical percutaneous facial nerve stimulation and recording of compound motor action potentials can be used to map the facial nerve branches. During surgery, the nerve map and continuous intraoperative motor end plate potential monitoring can be used to reduce nerve injury.
Objective: To investigate if preoperative facial nerve mapping (FNM) is associated with intraoperative facial nerve injury risk and safe surgical approach options compared with standard nerve integrity monitoring (NIM).
Design, setting, and participants: This investigation was a historically controlled study at a tertiary vascular anomaly center in Seattle, Washington. Participants were 92 pediatric patients with facial vascular anomalies undergoing definitive anomaly surgery (from January 1, 1999, through January 1, 2015), with 2 years' follow-up. In retrospective review, a consecutive FNM patient cohort after 2005 (FNM group) was compared with a consecutive historical cohort (1999-2005) (NIM group).
Main outcomes and measures: Postoperative facial nerve function and selected surgical approach. For NIM and FNM comparisons, statistical analysis calculated odds ratios of nerve injury and operative approach, and time-to-event methods analyzed operative time.
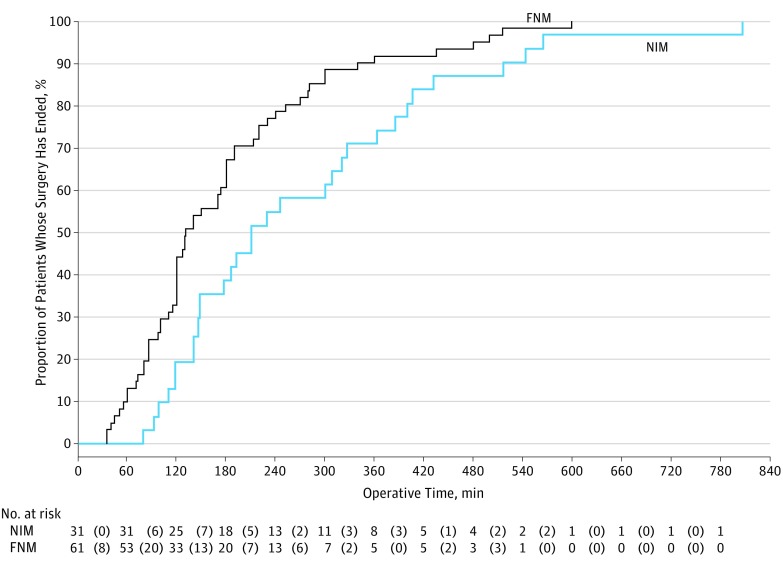
Results: The NIM group had 31 patients (median age, 3.3 years [interquartile range, 2.2-11.4 years]; 20 [65%] male), and the FNM group had 61 patients (median age, 4.4 years [interquartile range, 1.5-11.0 years]; 26 [43%] male). In both groups, lymphatic malformation resection was most common (19 of 31 [61%] in the NIM group and 32 of 61 [52%] in the FNM group), and the median anomaly volumes were similar (52.4 mL; interquartile range, 12.8-183.3 mL in the NIM group and 65.4 mL; interquartile range, 18.8-180.2 mL in the FNM group). Weakness in the facial nerve branches at 2 years after surgery was more common in the NIM group (6 of 31 [19%]) compared with the FNM group (1 of 61 [2%]) (percentage difference, 17%; 95% CI, 3%-32%). Anterograde facial nerve dissection was used more in the NIM group (27 of 31 [87%]) compared with the FNM group (28 of 61 [46%]) (percentage difference, 41%; 95% CI, 24%-58%). Treatment with retrograde dissection without identification of the main trunk of the facial nerve was performed in 21 of 61 (34%) in the FNM group compared with 0 of 31 (0%) in the NIM group. Operative time was significantly shorter in the FNM group, and patients in the FNM group were more likely to complete surgery sooner (adjusted hazard ratio, 5.36; 95% CI, 2.00-14.36).
Conclusions and relevance: Facial nerve mapping before facial vascular anomaly surgery was associated with less intraoperative facial nerve injury and shorter operative time. Mapping enabled direct identification of individual intralesional and perilesional nerve branches, reducing the need for traditional anterograde facial nerve dissection, and allowed for safe removal of some lesions after partial nerve dissection through transoral or direct excision.
Conflict of interest statement
Figures


Similar articles
-
Facial Nerve Branching Patterns Vary With Vascular Anomalies.Laryngoscope. 2020 Nov;130(11):2708-2713. doi: 10.1002/lary.28500. Epub 2020 Jan 11. Laryngoscope. 2020. PMID: 31925962
-
Association Between Facial Nerve Monitoring With Postoperative Facial Paralysis in Parotidectomy.JAMA Otolaryngol Head Neck Surg. 2016 Sep 1;142(9):828-33. doi: 10.1001/jamaoto.2016.1192. JAMA Otolaryngol Head Neck Surg. 2016. PMID: 27310887
-
Additional Benefits of Facial Nerve Monitoring during Otologic Surgery.Otolaryngol Head Neck Surg. 2020 Sep;163(3):572-576. doi: 10.1177/0194599820915458. Epub 2020 Apr 14. Otolaryngol Head Neck Surg. 2020. PMID: 32283984
-
Proposals for Standardization of Intraoperative Facial Nerve Monitoring during Parotid Surgery.Diagnostics (Basel). 2022 Sep 30;12(10):2387. doi: 10.3390/diagnostics12102387. Diagnostics (Basel). 2022. PMID: 36292076 Free PMC article. Review.
-
Best Practices in Facial Nerve Monitoring.Laryngoscope. 2021 Apr;131 Suppl 4:S1-S42. doi: 10.1002/lary.29459. Laryngoscope. 2021. PMID: 33729584 Review.
Cited by
-
Management of the facial nerve in parotid cancer: preservation or resection and reconstruction.Eur Arch Otorhinolaryngol. 2018 Nov;275(11):2615-2626. doi: 10.1007/s00405-018-5154-6. Epub 2018 Sep 28. Eur Arch Otorhinolaryngol. 2018. PMID: 30267218 Review.
-
Iatrogenic Facial Nerve Injury in Head and Neck Surgery in the Presence of Intraoperative Facial Nerve Monitoring With Electromyography: A Systematic Review.Cureus. 2023 Nov 6;15(11):e48367. doi: 10.7759/cureus.48367. eCollection 2023 Nov. Cureus. 2023. PMID: 38060739 Free PMC article. Review.
-
[Preservation, reconstruction, and rehabilitation of the facial nerve].HNO. 2023 Apr;71(4):232-242. doi: 10.1007/s00106-022-01148-y. Epub 2022 Mar 14. HNO. 2023. PMID: 35288765 Free PMC article. Review. German.
-
Facial nerve electrodiagnostics for patients with facial palsy: a clinical practice guideline.Eur Arch Otorhinolaryngol. 2020 Jul;277(7):1855-1874. doi: 10.1007/s00405-020-05949-1. Epub 2020 Apr 8. Eur Arch Otorhinolaryngol. 2020. PMID: 32270328 Free PMC article.
References
-
- Lee GS, Perkins JA, Oliaei S, Manning SC. Facial nerve anatomy, dissection and preservation in lymphatic malformation management. Int J Pediatr Otorhinolaryngol. 2008;72(6):759-766. - PubMed
-
- Slaughter KA, Chen T, Williams E III. Vascular lesions. Facial Plast Surg Clin North Am. 2016;24(4):559-571. - PubMed
-
- Hu X, Chen D, Jiang C, et al. . Retrospective analysis of facial paralysis caused by ethanol sclerotherapy for facial venous malformation. Head Neck. 2011;33(11):1616-1621. - PubMed
-
- Nyberg EM, Chaudry MI, Turk AS, Turner RD. Transient cranial neuropathies as sequelae of Onyx embolization of arteriovenous shunt lesions near the skull base: possible axonotmetic traction injuries. J Neurointerv Surg. 2013;5(4):e21. - PubMed
-
- de Serres LM, Sie KC, Richardson MA. Lymphatic malformations of the head and neck: a proposal for staging. Arch Otolaryngol Head Neck Surg. 1995;121(5):577-582. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
