

Quantification of an Exercise Rehabilitation Program for Severely Burned Children: The Standard of Care at Shriners Hospitals for Children®-Galveston
- PMID: 29596648
- PMCID: PMC6060021
- DOI: 10.1093/jbcr/iry001
Quantification of an Exercise Rehabilitation Program for Severely Burned Children: The Standard of Care at Shriners Hospitals for Children®-Galveston
Abstract
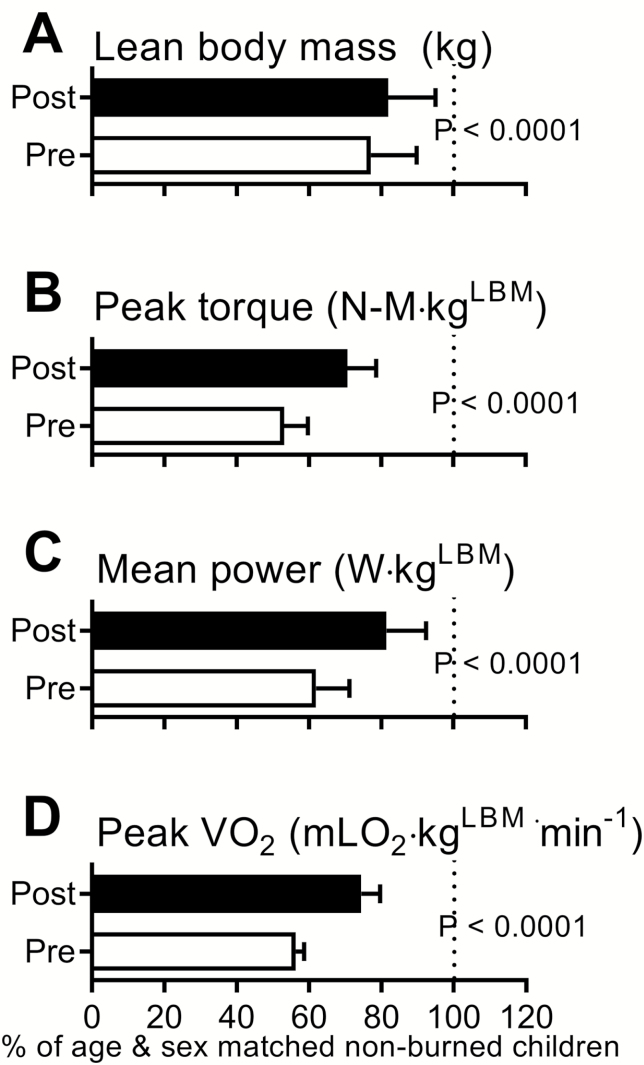
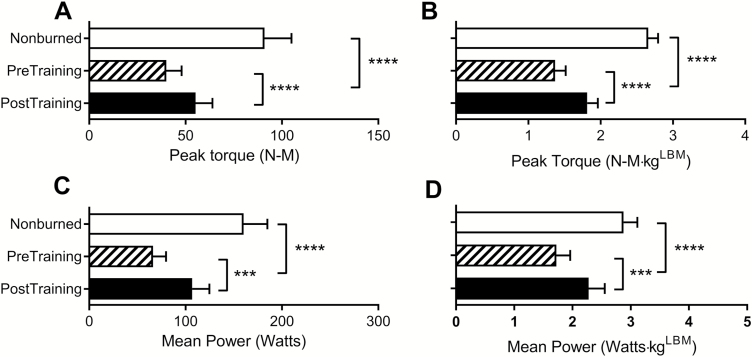
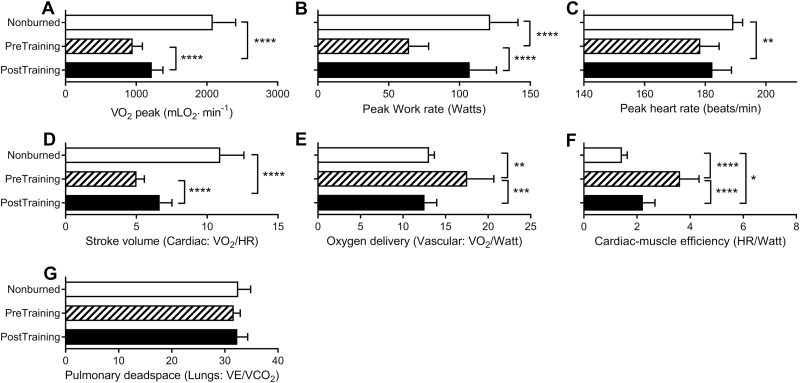
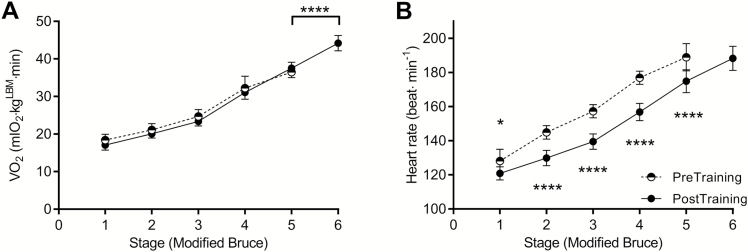
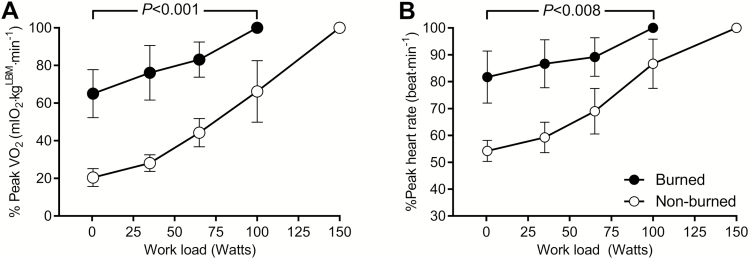
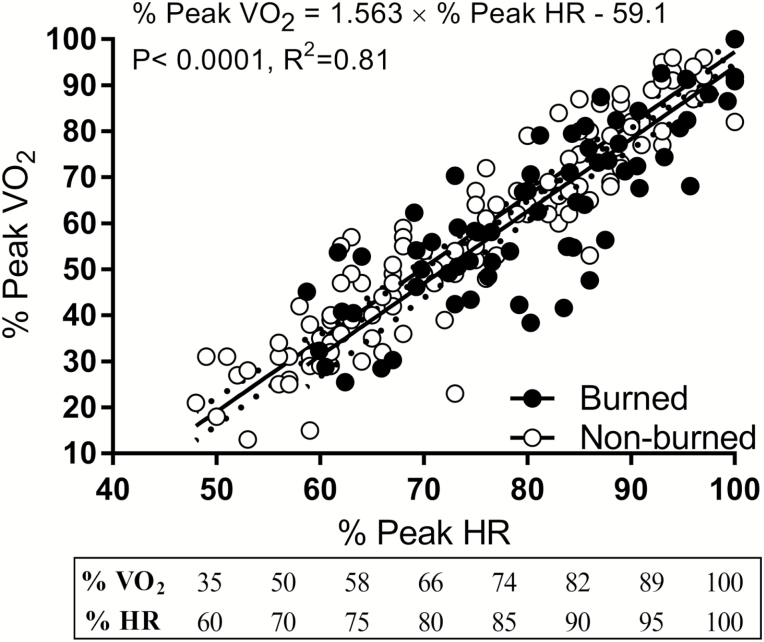
Currently, there are no clear guidelines for the implementation of rehabilitative exercise training (RET) in burned individuals. Therefore, we quantified the training logs for exercise intensity, frequency, and duration of 6 weeks of this program to develop a basic framework for outpatient RET in patients recovering from severe burns. Thirty-three children (11 female, [mean ± SD] 12 ± 3 years, 145 ± 18 cm, 40 ± 11 kg, 49 ± 31 BMI percentile) with severe burns (49 ± 15% total body surface area burned, with 35 ± 22% third-degree burns) completed our 6-week resistance and aerobic exercise training program. Cardiorespiratory fitness (peak VO2), strength, power, and lean body mass (LBM) were measured before and after RET. Outcome measures were analyzed as a relative percentage of values in age- and sex-matched nonburned children (11 female, 12 ± 3 years, 154 ± 20 cm, 49 ± 22 kg, 56 ± 25 BMI percentile). At discharge, burned children had lower LBM (77% of age-sex-matched nonburn values), peak torque (53%), power (62%), and cardiorespiratory fitness (56%). After 6 weeks of training, LBM increased by 5% (82% of nonburn values), peak torque by 18% (71%), power by 20% (81%), and cardiorespiratory fitness by 18% (74%; P < .0001 for all). Quantification of data in exercise training logs suggested that physical capacity can be improved by aerobic exercise training performed at five metabolic equivalents (>70% of peak VO2) at least 3 days/week and 150 minutes/week and by resistance training performed at volume loads (reps × sets × weight) of 131 kg for the upper body and 275 kg for the lower body for 2 days/week. We present for the first time the quantification of our RET and provide clear exercise prescription guidelines specific to children with severe burn injury.
Figures
References
-
- World Health Organization. The global burden of disease: 2004 update. Geneva, Switzerland: 2008.
-
- Shields BJ, Comstock RD, Fernandez SA, Xiang H, Smith GA. Healthcare resource utilization and epidemiology of pediatric burn-associated hospitalizations, United States, 2000. J Burn Care Res 2007;28:811–826. - PubMed
-
- Gibran NS, Wiechman S, Meyer W, et al. Summary of the 2012 ABA burn quality consensus conference. J Burn Care Res 2013;34:361–385. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
