

Psychological outcomes and surgical decisions after genetic testing in women newly diagnosed with breast cancer with and without a family history
- PMID: 29599518
- PMCID: PMC6018744
- DOI: 10.1038/s41431-017-0057-3
Psychological outcomes and surgical decisions after genetic testing in women newly diagnosed with breast cancer with and without a family history
Abstract
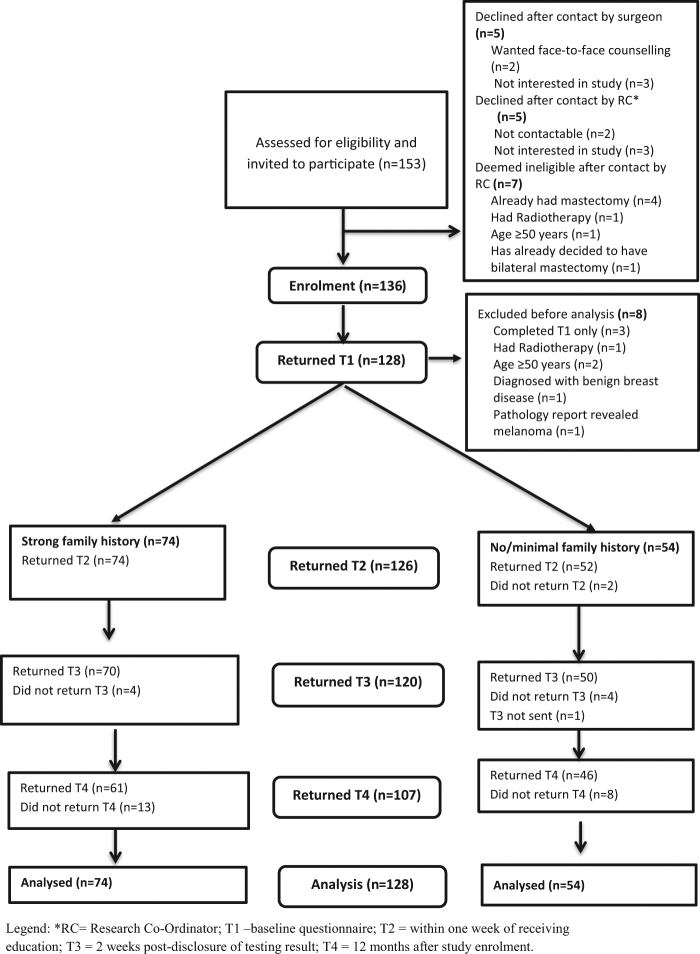
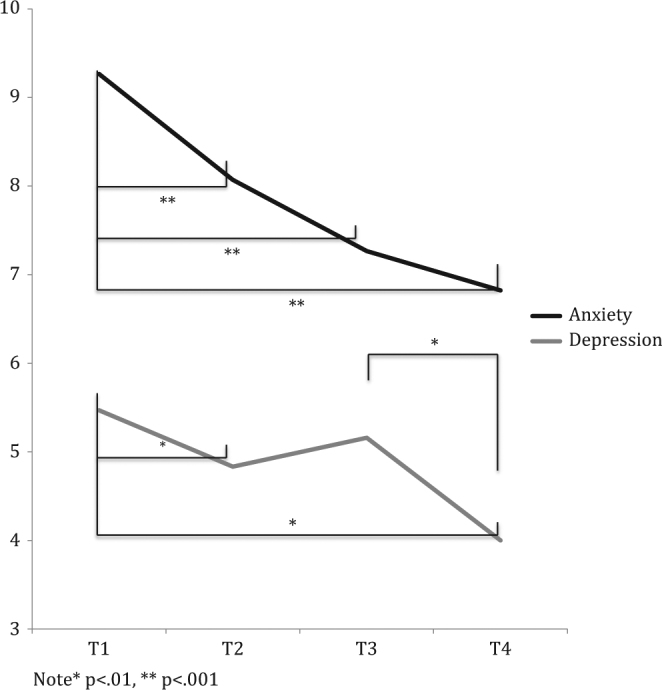
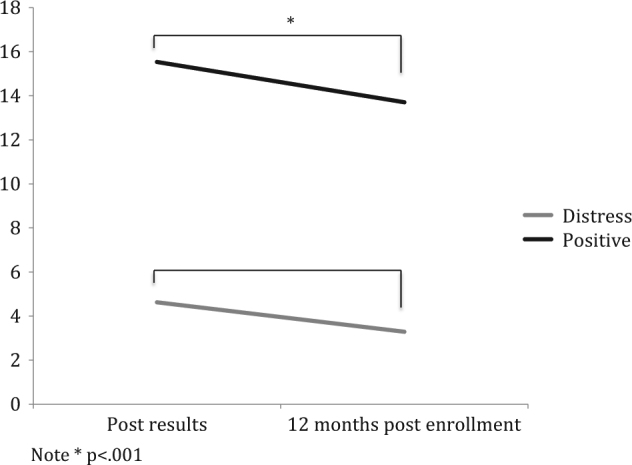
In patients with early breast cancer, personal and tumour characteristics other than family history are increasingly used to prompt genetic testing to guide women's cancer management (treatment-focused genetic testing, 'TFGT'). Women without a known strong family history of breast and/or ovarian may be more vulnerable to psychological sequelae arising from TFGT. We compared the impact of TFGT in women with (FH+) and without (FH-) a strong family history on psychological adjustment and surgical decisions. Women aged <50 years with high-risk features were offered TFGT before definitive breast cancer surgery and completed self-report questionnaires at four time points over 12 months. All 128 women opted for TFGT. TFGT identified 18 carriers of a disease-causing variant (50.0% FH+) and 110 non-carriers (59.1% FH+). There were no differences based on family history in bilateral mastectomy (BM) uptake, p = .190, or uptake of risk-reducing bilateral salpingo-oophorectomy (RRBSO), p = .093. FH- women had lower decreases in anxiety a year after diagnosis, p = .011, and regret regarding their decision whether to undergo BM, p = .022, or RRBSO, p = .016 than FH + women. FH- carriers reported significantly higher regret regarding their TFGT choice (p = .024) and test-related distress (p = .012) than FH + carriers, but this regret/distress could not be attributed to a concern regarding a possible worse prognosis. These findings indicate that FH- women may require additional counselling to facilitate informed decisions. Carriers without a family history may require additional follow-up counselling to facilitate psychological adjustment to their positive variant results, extra support in making surgical decisions, and counselling about how best to communicate results to family members.
Conflict of interest statement
BM, KT and MG have remunerated consultant roles with the company Astrazeneca with respect to unrelated projects. The remaining authors declare that they have no competing intersts.
Figures
Similar articles
-
When knowledge of a heritable gene mutation comes out of the blue: treatment-focused genetic testing in women newly diagnosed with breast cancer.Eur J Hum Genet. 2016 Nov;24(11):1517-1523. doi: 10.1038/ejhg.2016.69. Epub 2016 Jun 22. Eur J Hum Genet. 2016. PMID: 27329735 Free PMC article.
-
Streamlined genetic education is effective in preparing women newly diagnosed with breast cancer for decision making about treatment-focused genetic testing: a randomized controlled noninferiority trial.Genet Med. 2017 Apr;19(4):448-456. doi: 10.1038/gim.2016.130. Epub 2016 Sep 29. Genet Med. 2017. PMID: 27684037 Clinical Trial.
-
How should we discuss genetic testing with women newly diagnosed with breast cancer? Design and implementation of a randomized controlled trial of two models of delivering education about treatment-focused genetic testing to younger women newly diagnosed with breast cancer.BMC Cancer. 2012 Jul 28;12:320. doi: 10.1186/1471-2407-12-320. BMC Cancer. 2012. PMID: 22838957 Free PMC article. Clinical Trial.
-
Hormone therapy after prophylactic risk-reducing bilateral salpingo-oophorectomy in women who have BRCA gene mutation.Climacteric. 2016 Oct;19(5):419-22. doi: 10.1080/13697137.2016.1209396. Epub 2016 Jul 16. Climacteric. 2016. PMID: 27426853 Review.
-
Family history as a predictor of uptake of cancer preventive procedures by women with a BRCA1 or BRCA2 mutation.Clin Genet. 2008 May;73(5):474-9. doi: 10.1111/j.1399-0004.2008.00988.x. Epub 2008 Mar 12. Clin Genet. 2008. PMID: 18341607 Review.
Cited by
-
Patient-Reported Outcomes following Genetic Testing for Familial Hypercholesterolemia, Breast and Ovarian Cancer Syndrome, and Lynch Syndrome: A Systematic Review.J Pers Med. 2021 Aug 27;11(9):850. doi: 10.3390/jpm11090850. J Pers Med. 2021. PMID: 34575627 Free PMC article. Review.
-
Psychosocial outcome and health behaviour intent of breast cancer patients with BRCA1/2 and PALB2 pathogenic variants unselected by a priori risk.PLoS One. 2022 Feb 15;17(2):e0263675. doi: 10.1371/journal.pone.0263675. eCollection 2022. PLoS One. 2022. PMID: 35167615 Free PMC article.
-
Hereditary Gastric and Breast Cancer Syndromes Related to CDH1 Germline Mutation: A Multidisciplinary Clinical Review.Cancers (Basel). 2020 Jun 17;12(6):1598. doi: 10.3390/cancers12061598. Cancers (Basel). 2020. PMID: 32560361 Free PMC article. Review.
-
Universal genetic testing for women with newly diagnosed breast cancer in the context of multidisciplinary team care.Med J Aust. 2023 May 1;218(8):368-373. doi: 10.5694/mja2.51906. Epub 2023 Apr 2. Med J Aust. 2023. PMID: 37005005 Free PMC article.
-
Heterogeneity of posttraumatic stress, depression, and fear of cancer recurrence in breast cancer survivors: a latent class analysis.J Cancer Surviv. 2023 Oct;17(5):1510-1521. doi: 10.1007/s11764-022-01195-y. Epub 2022 Feb 28. J Cancer Surviv. 2023. PMID: 35224684 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
